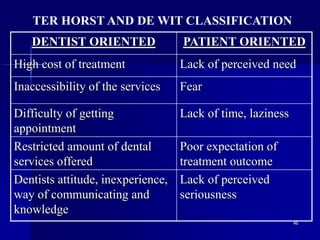
The document discusses barriers to utilization of dental health care services. It defines key terms like need, health services, utilization, and barriers. It then describes various factors that can act as barriers, such as age, gender, race, education level, income level, dental insurance coverage, and geographic location. Barriers are also classified in different ways by various researchers, such as availability, accessibility, affordability, acceptability and accommodation of services. Common barriers include cost of treatment, fear or anxiety associated with dental procedures, lack of perceived need for care, and lack of access to dental services and insurance coverage.







![125
Challenges to the Oral Health Workforce in
India; Shobha Tandon; Journal of Dental
Education, Volume 68, Number 7 Supplement
Access to Social Services by the Poor and
Disadvantaged in Asia and the Pacific; III.
Determining Needs
Overcoming barriers in public health
communications in India; Ewing M; Source:
Information & Knowledge for Optimal Health
(INFO) Project; 1989. [5], 194, [5] p.](https://image.slidesharecdn.com/barriersseminarfinal-230710154833-5753bb43/85/barriers-seminar-final-ppt-125-320.jpg)
































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)









