Downloaded 16 times





![Human and Animal Histology/Immunohistochemistry Core
• VCA clinical samples (>2000)
– Tissue samples: muscle, skin, tendon, nerve, artery, vein
• Histopathology Core
• Digital Library
– Digital slide scanning – Aperio AT [400 slide scan capability]
• Dedicated Lab Space
• Histology Staff
Digital Library](https://image.slidesharecdn.com/banffvcaconsensusstatemetlcendalessenttokim-151009211755-lva1-app6892/85/Banff-vca-consensus-statemet-l-cendales-sent-to-kim-39-320.jpg)

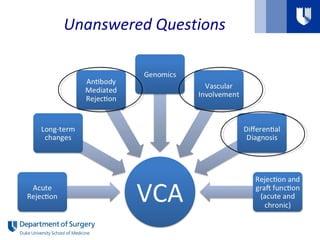
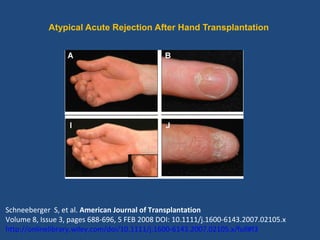
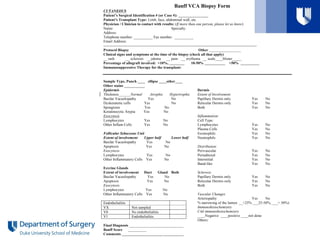
The document summarizes discussions from a workshop on vascularized composite allotransplantation (VCA) pathology. It addresses several unanswered questions in the field and proposes updates to the Banff VCA classification system. Key points discussed include: - Reviewing the specificity and significance of isolated dyskeratotic/apoptotic cells in different skin structures for grading rejection. - Studying the roles of C4d staining, antibody functions, and chronic changes like vasculopathy. - Addressing questions from an AST working group on expanding grading criteria, differences between hand and face transplants, optimal biopsy size and location. - Proposing a standardized biopsy collection form and digital library to facilitate



































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










