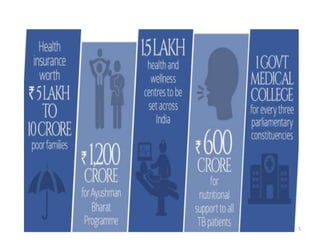
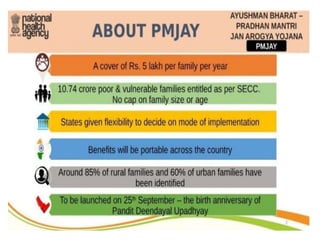
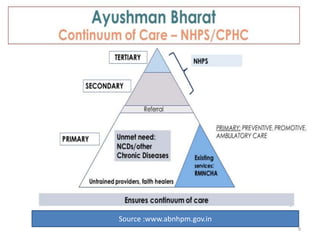
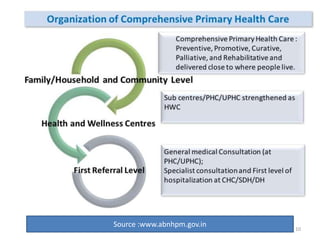
This document provides an overview of Ayushman Bharat, the national health protection mission of India. It discusses the rationale for Ayushman Bharat, which aims to provide comprehensive primary, secondary and tertiary healthcare through two major components: Health and Wellness Centers and the Pradhan Mantri Jan Arogya Yojana (PM-JAY). The key initiatives discussed include establishing 150,000 Health and Wellness Centers across India to provide comprehensive primary healthcare, and PM-JAY which provides health insurance coverage to over 100 million poor and vulnerable families for secondary and tertiary care.





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















