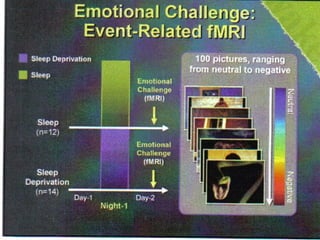
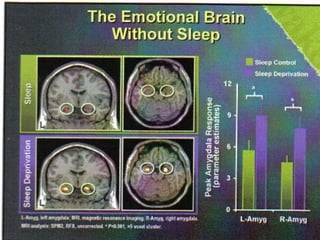
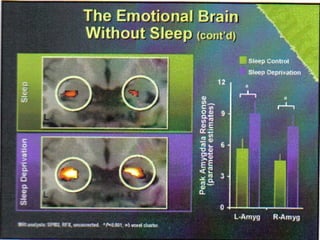
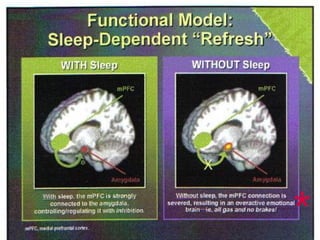
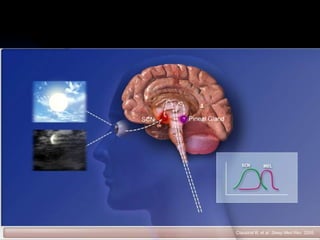
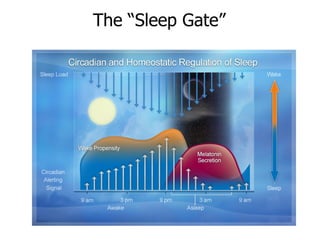
Sleep is important for memory consolidation and emotional regulation. Lack of sleep can impair memory formation and exaggerate emotional reactions by overactivating the amygdala. The brain's master clock is located in the hypothalamus and regulates circadian rhythms, with light being the main synchronizing cue. Disruptions to circadian rhythms and sleep disturbances are associated with mood disorders like depression. Chronotherapy approaches like light therapy and sleep scheduling can help treat mood disorders by realigning circadian rhythms.