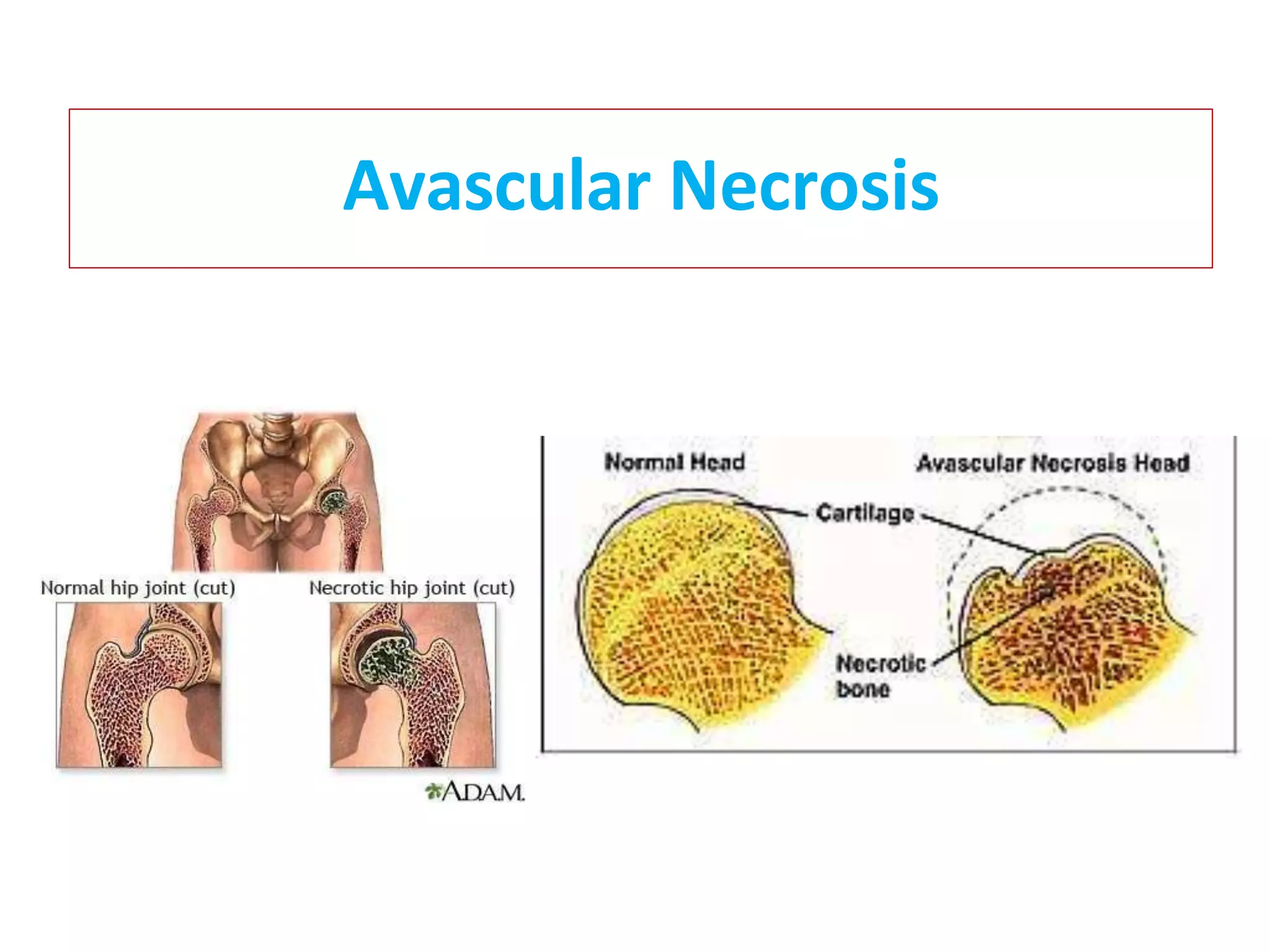
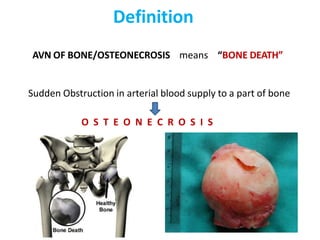
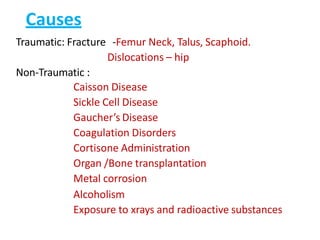
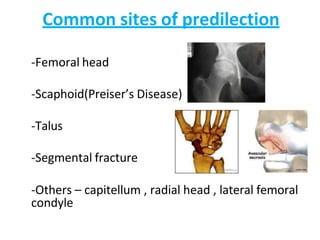
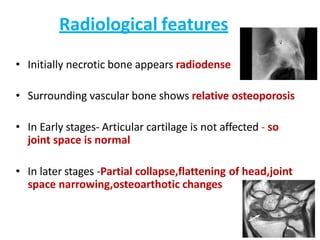
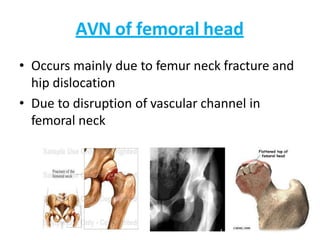
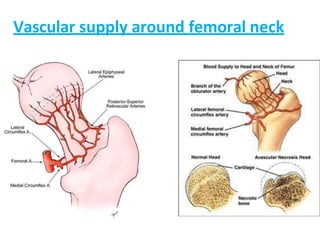
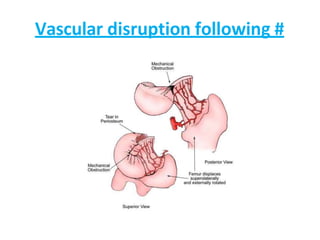
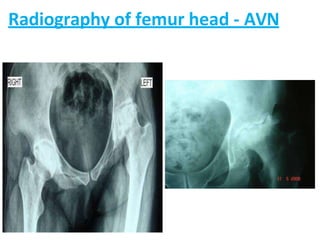
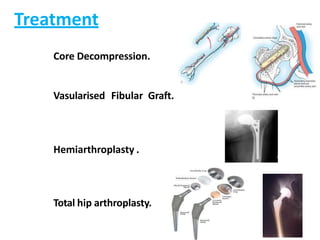
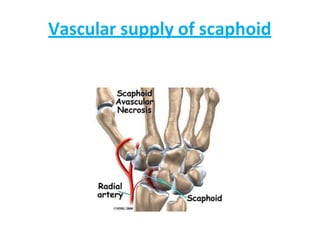
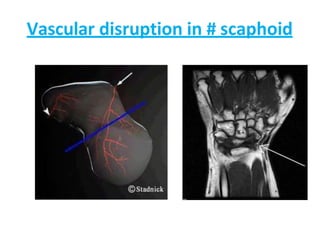
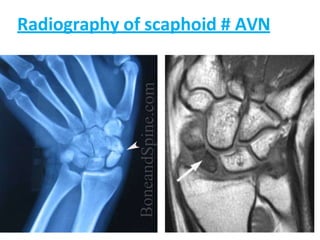
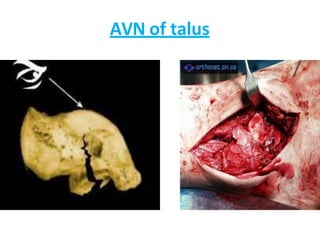
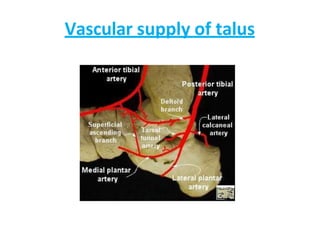
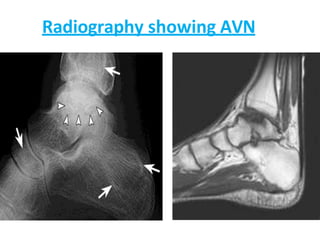
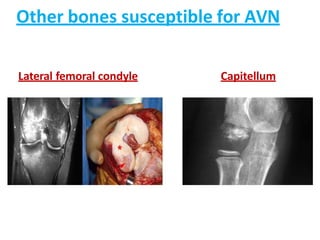
This document discusses avascular necrosis (AVN), also known as osteonecrosis or bone death. It defines AVN as the sudden obstruction of arterial blood supply to bone. Common causes include trauma, corticosteroid use, and decompression sickness. Sites commonly affected are the femoral head, scaphoid, and talus. The goal of treatment is to improve joint function, stop further bone damage, and preserve the bone and joint. Methods include nonsurgical options to delay progression and surgical interventions like core decompression or grafts, with arthroplasty reserved for later stages.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

