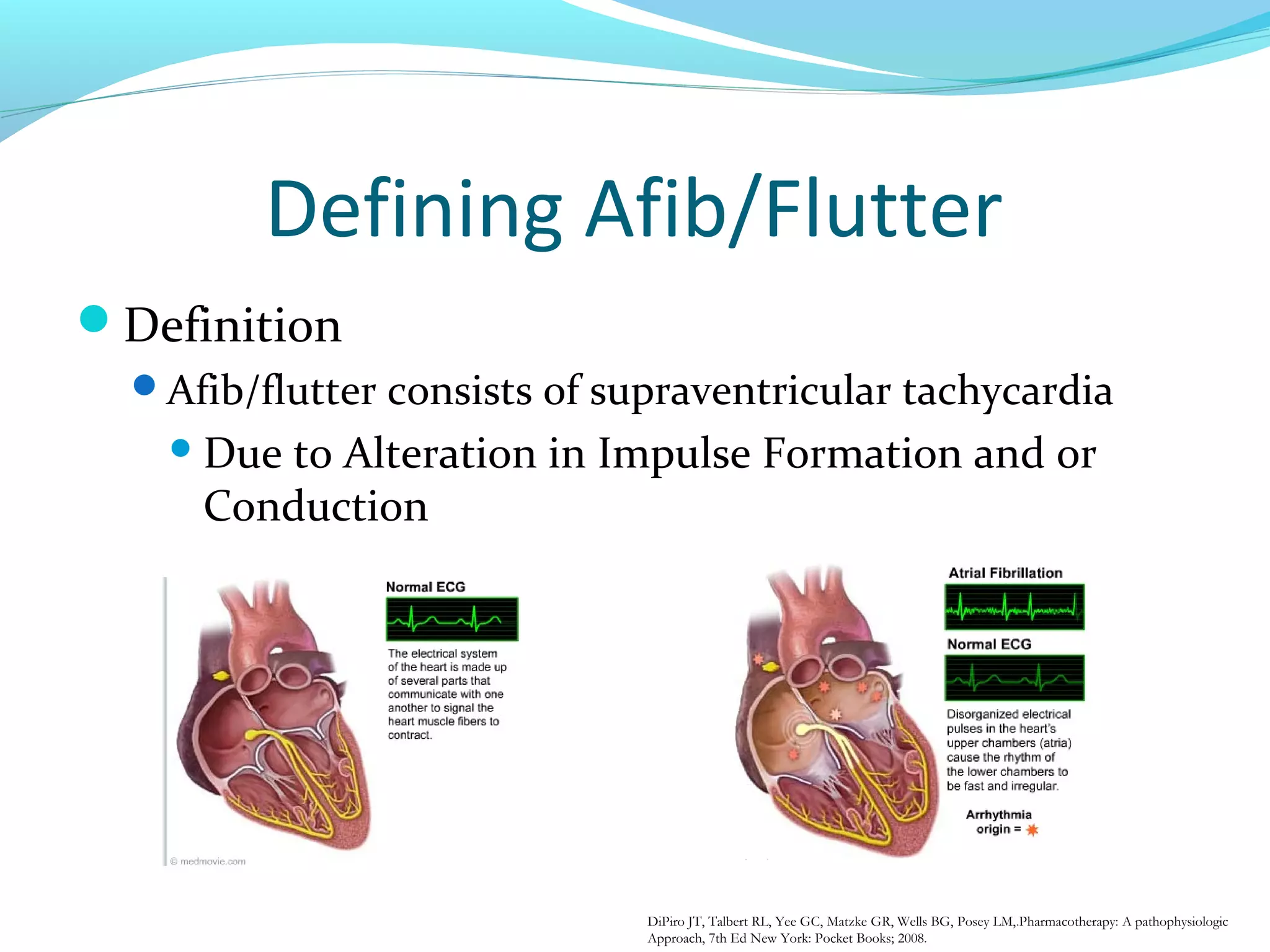
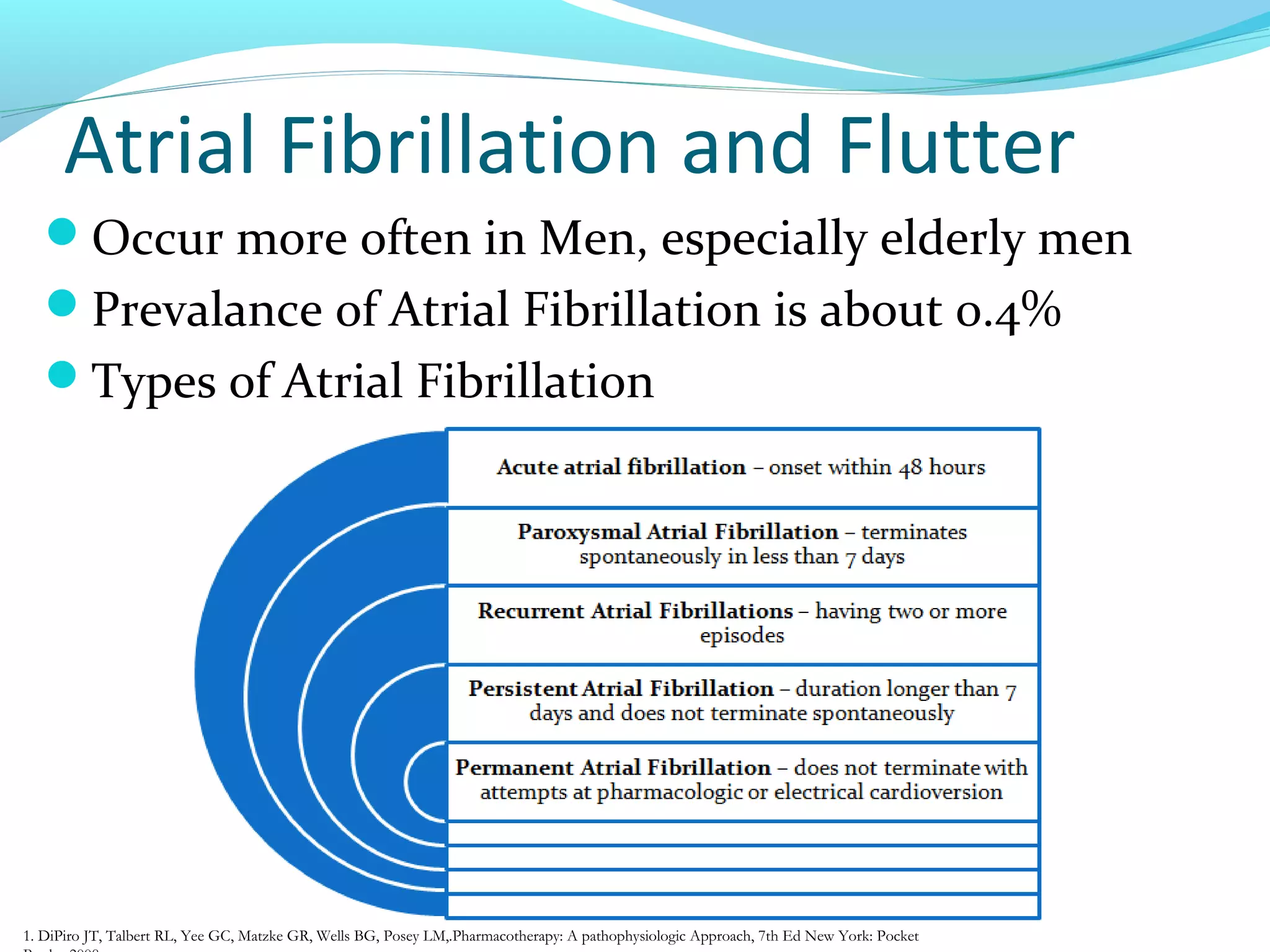
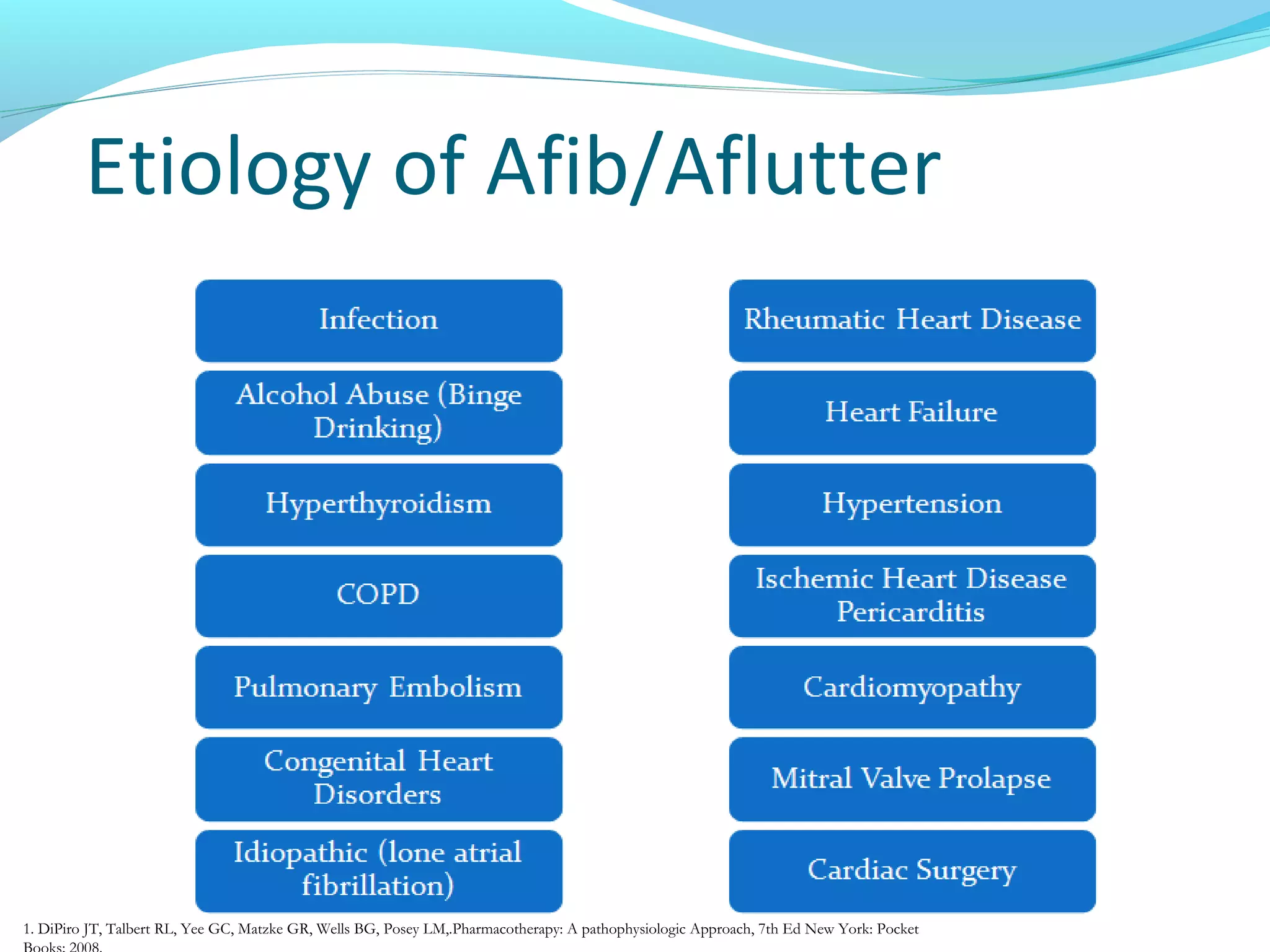
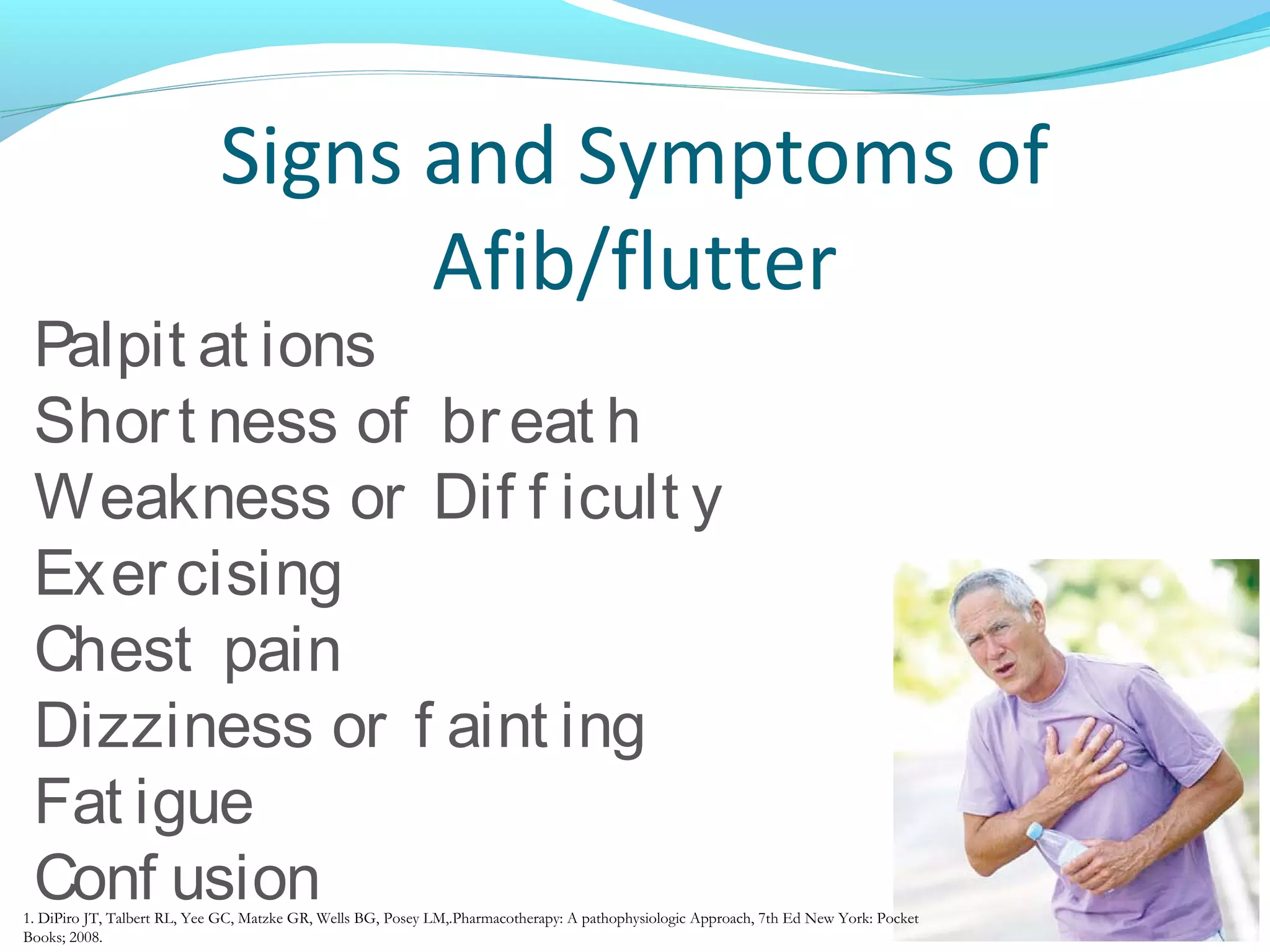
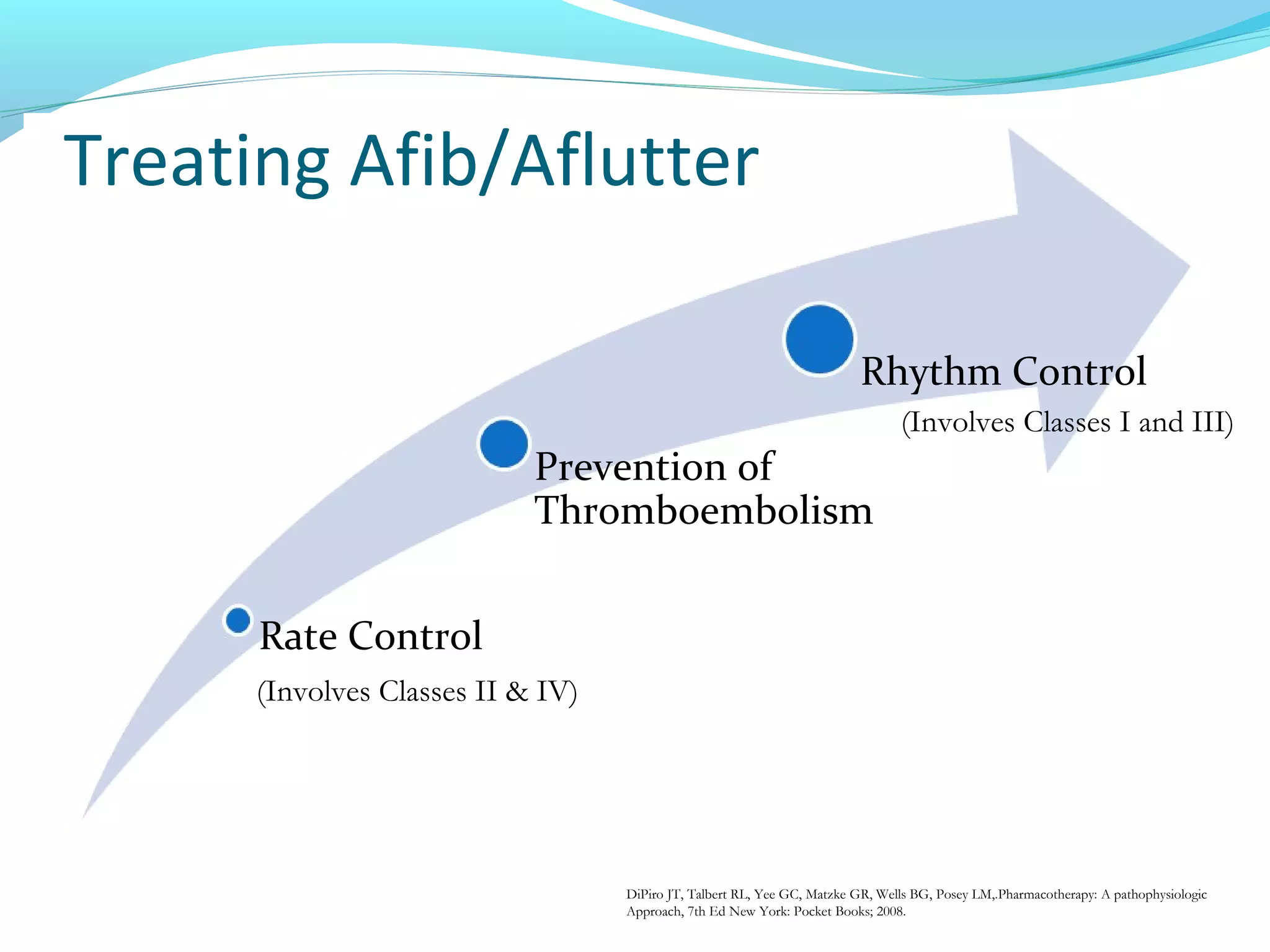
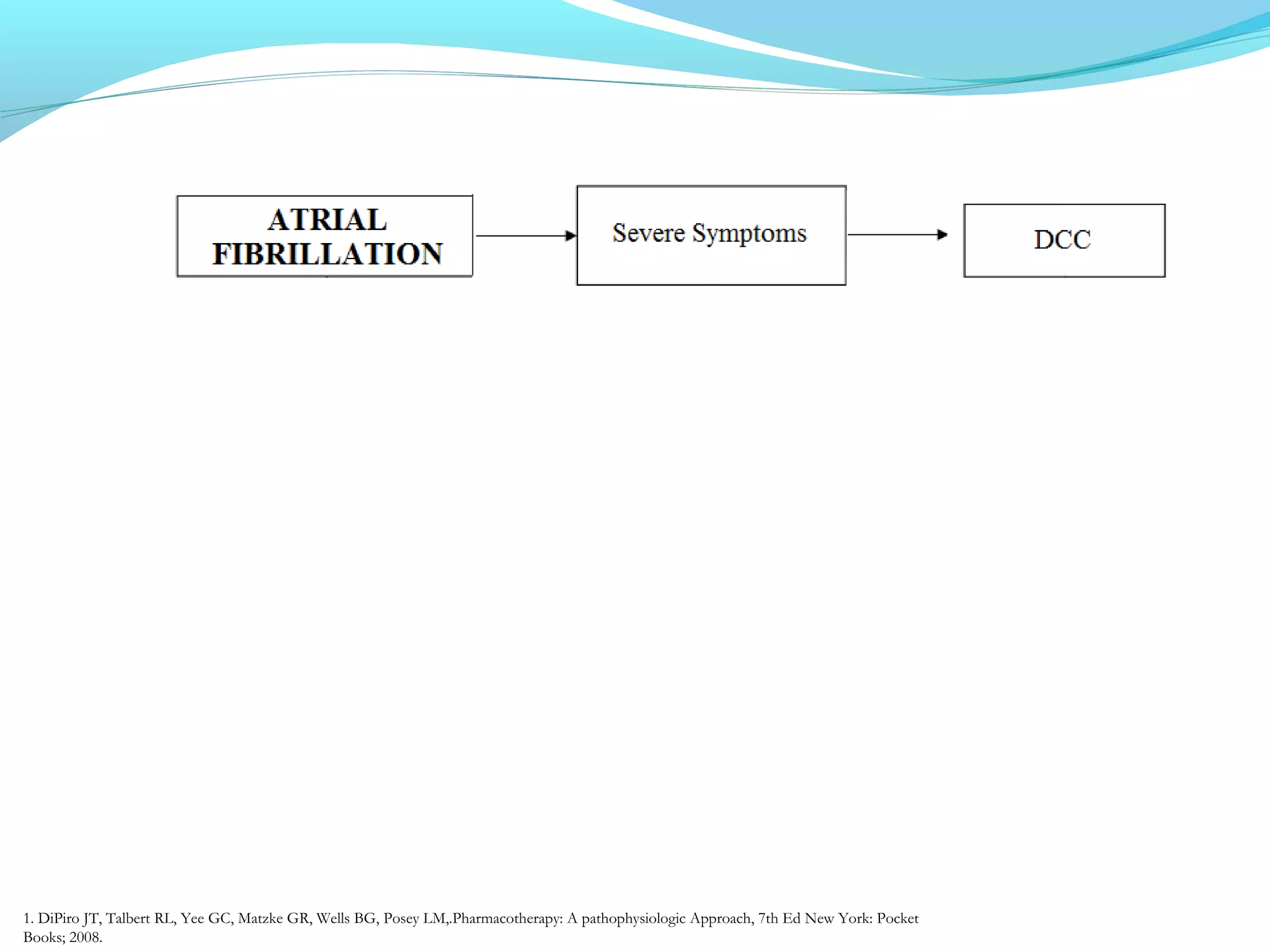
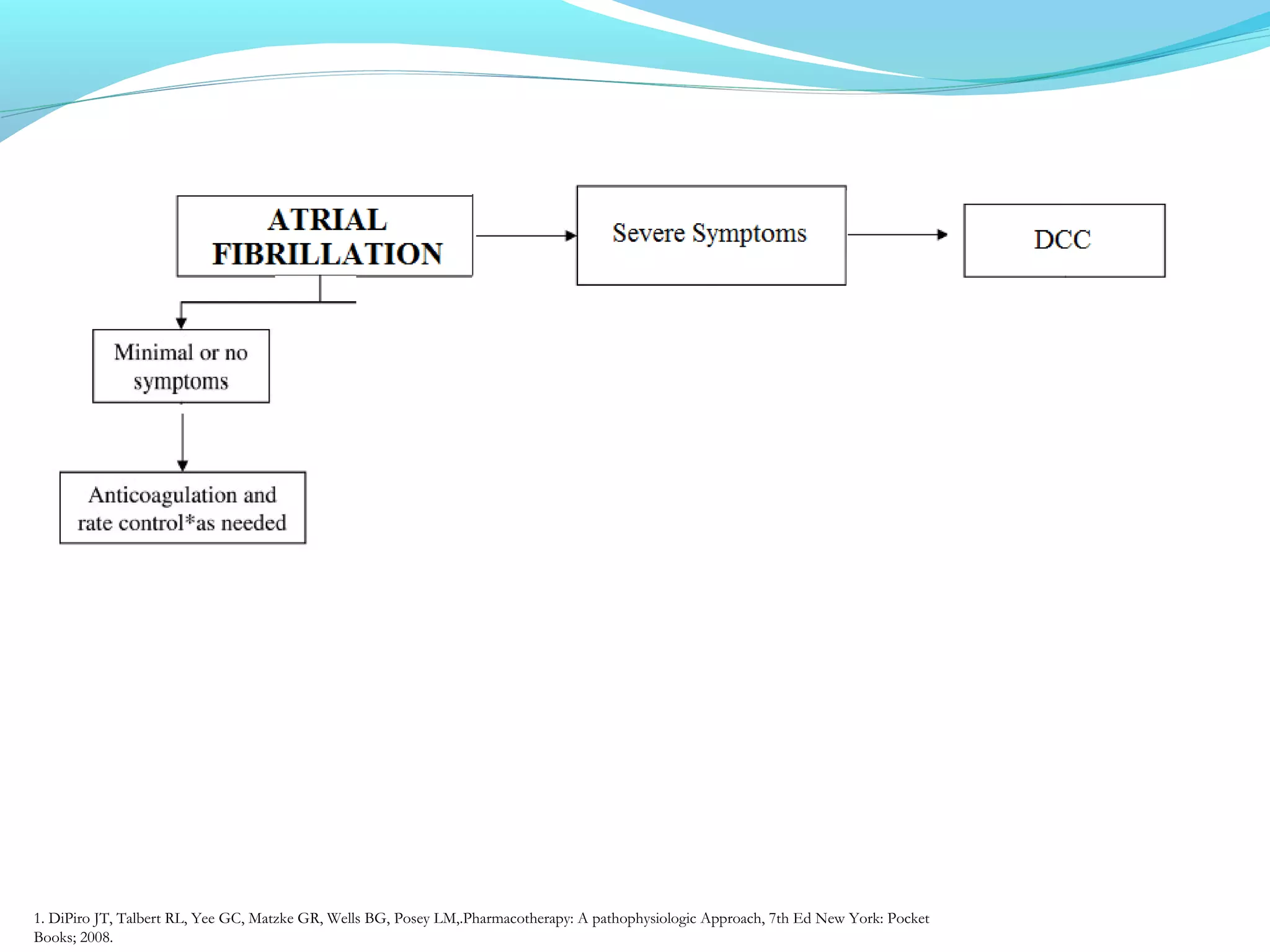
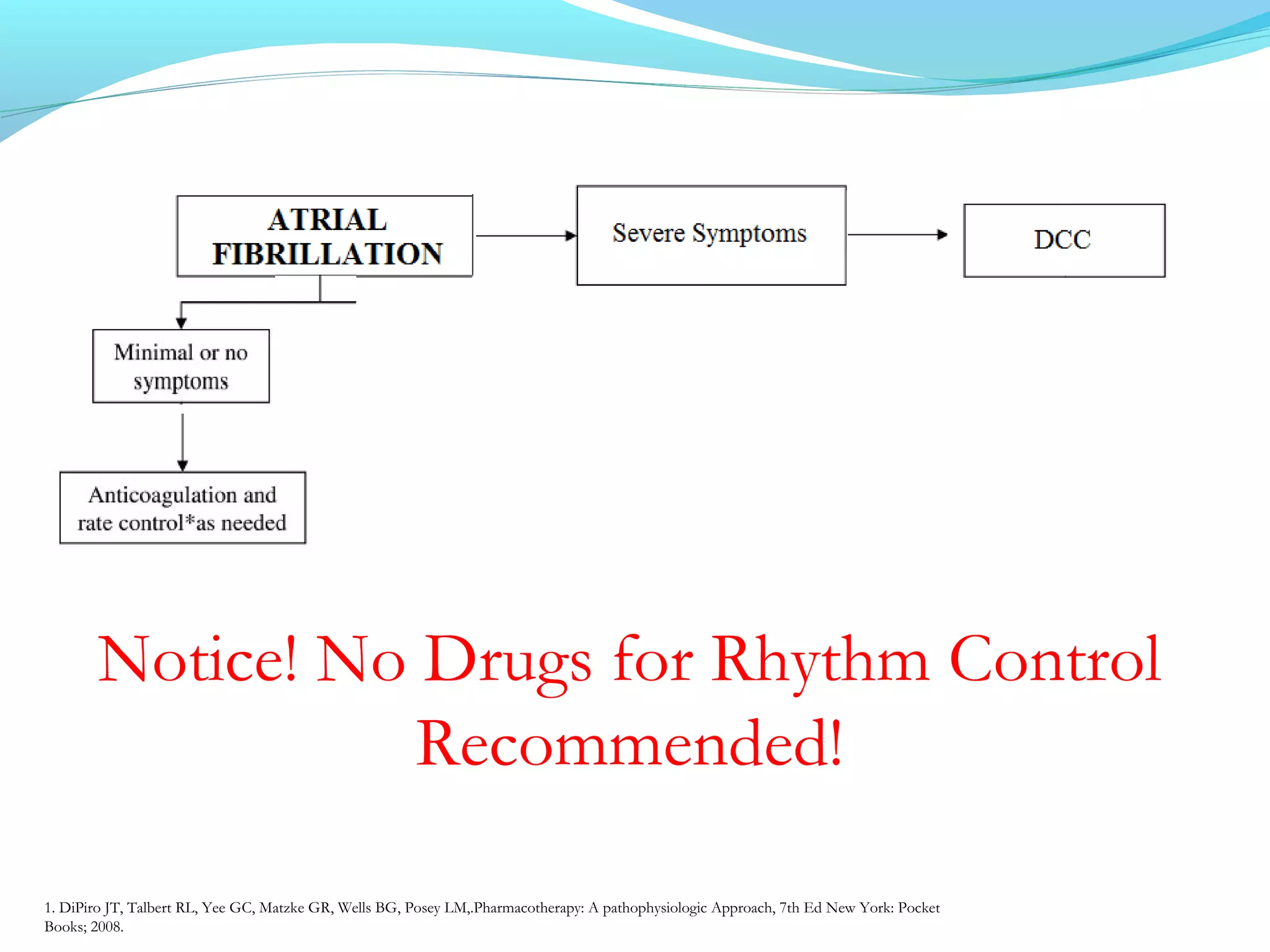
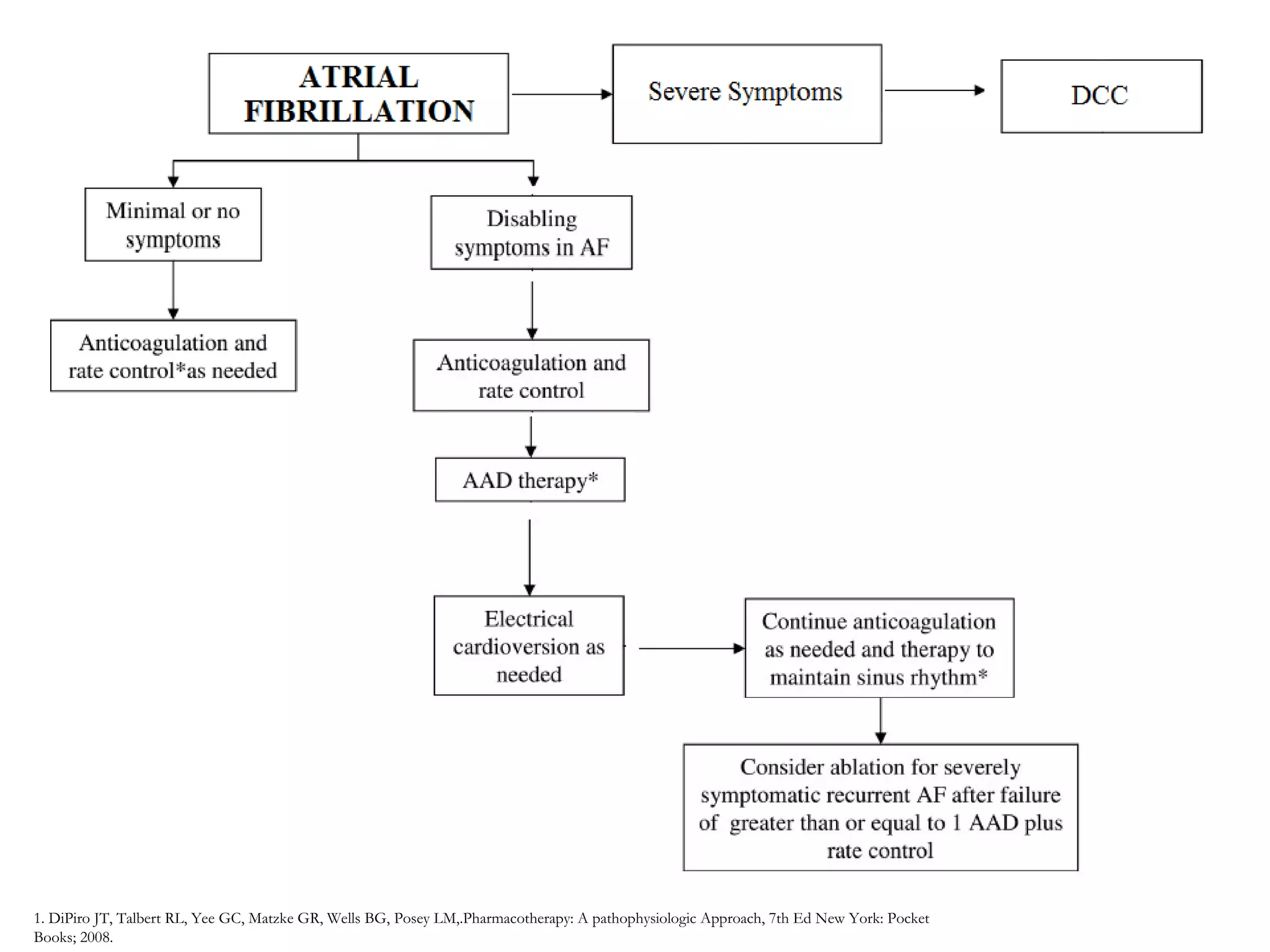
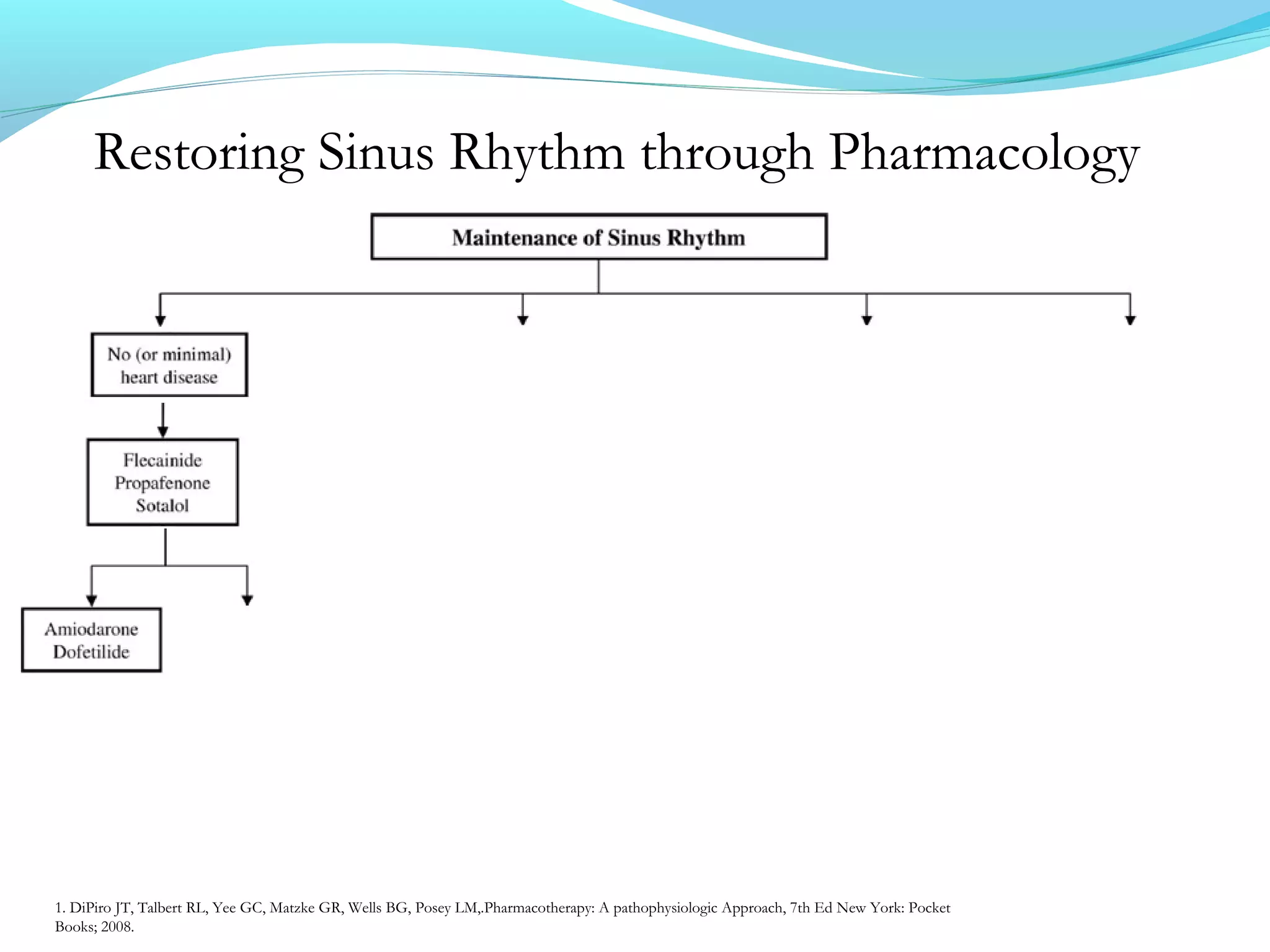
This document summarizes atrial fibrillation (Afib) and atrial flutter, including definitions, types, causes, symptoms, and treatment approaches. Afib and flutter are types of abnormal heart rhythms that involve rapid and irregular beating of the upper chambers of the heart. Treatment involves rate control to regulate heart rate, prevention of blood clots, and in some cases restoring normal rhythm through cardioversion or antiarrhythmic drugs. The document reviews medications and procedures for treating Afib and flutter based on severity of symptoms.