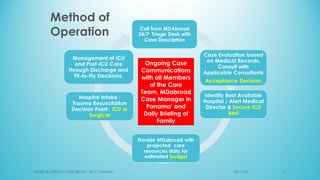
The document presents a case report from Neuro & Critical Care (NCC) based in Panama, focusing on two critical trauma cases—a traumatic brain injury and a gunshot wound. It details the medical assessments, treatment protocols, and recommendations for both patients, highlighting the multidisciplinary approach of the NCC team in managing life-threatening conditions. The report underscores the importance of ongoing care communication, therapy, and rehabilitation for optimal recovery outcomes.