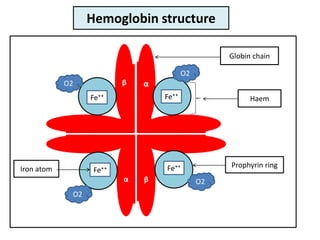
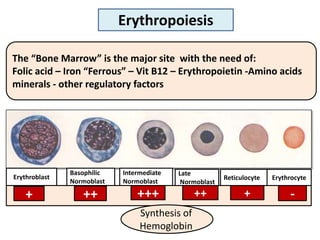
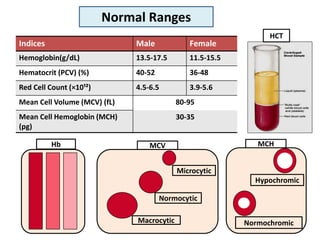
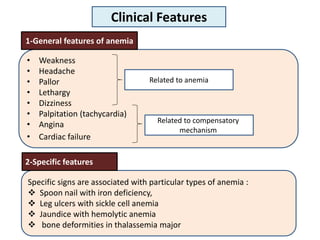
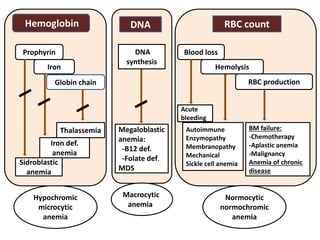
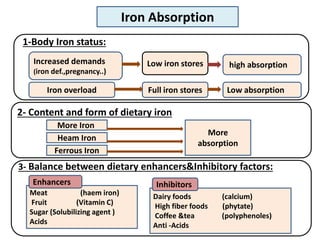
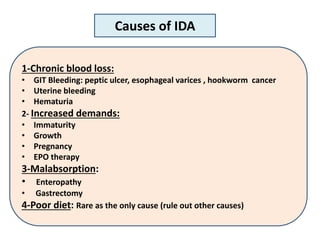
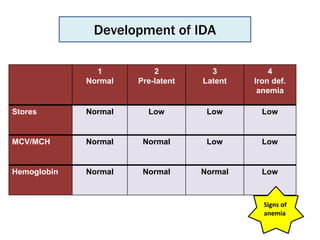
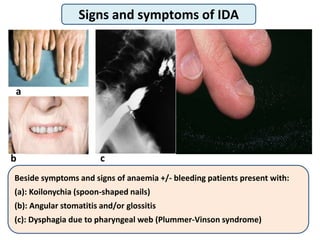
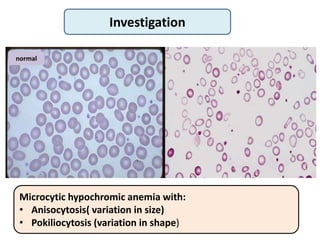
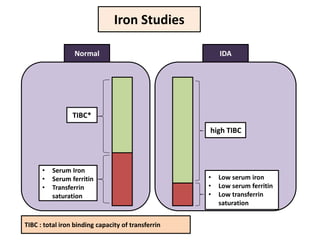
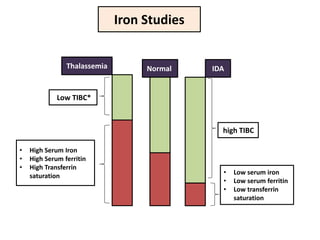
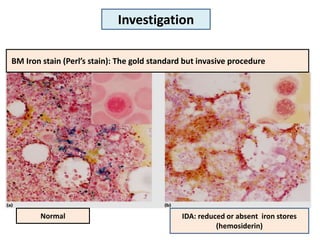
Anemia is a reduction in hemoglobin concentration below the normal range due to decreased oxygen-carrying capacity of blood. Hemoglobin in red blood cells transports oxygen from the lungs to tissues and carbon dioxide back. Iron deficiency anemia is the most common type and results from chronic blood loss or increased demands exceeding iron absorption. It causes microcytic hypochromic anemia and is diagnosed through blood tests showing low iron, ferritin and transferrin saturation. Treatment involves iron replacement therapy and treating the underlying cause.





























![PhD_sensitization__slides[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/phdsensitizationslides1-231105112926-fe565658-thumbnail.jpg?width=640&height=640&fit=bounds)


























