
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Andrea oligodendroglioma
Similar to Andrea oligodendroglioma (20)
Recently uploaded
Recently uploaded (20)
Andrea oligodendroglioma
- 1. http://www.pubcan.org/cancer/18/oligodendroglioma-nos/histopathology http://radiographics.rsna.org/content/25/6/1669/F28.expansion.html Andrea Laszczyk
- 2. Found anywhere oligodendrocytes are. http://science-naturalphenomena.blogspot.com.au/2009/04/oligodendrocytes.html Most commonly found in cerebral hemispheres Relatively slow growing Rarely spread outside CNS Drop mets 1-2% of the time
- 3. 2 – 5% of all brain tumours 5 – 33% of all Glial tumours Most common in 30 y.o. – 50 y.o. Rarely found in children M:F = 1.1 Only known aetiology, exposure to ioninsing radiation
- 5. MRI – in most cases CT – only if MRI contraindicated Biopsy Surgery Insight: the role of surgery in the management of low-grade gliomas Nader Pouratian, fNature Clinical Practice Neurology (2007) 3, 628-639
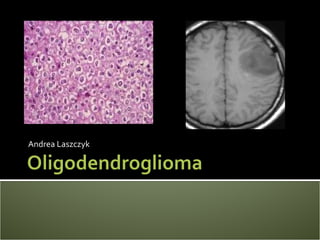
- 6. WHO guidelines rather than TNM Two tier system Grade II (77%) (left picture) Grade III(23%) (right picture) Grade II tumours can recur as Grade III tumours http://oligodendroglioma.org/ http://radiographics.rsna.org/content/25/6/1669/F2.expansion.html
- 7. Standard treatment approach – surgery Most often not fully resected RT alone, RT/Chemo or Chemo alone post surgery Watchful waiting
- 8. Mixed feelings on timing of RT use for treatment One EORTC study, 311 patients Immediate post operative RT Delayed RT ~8 years later Immediate RT = increased progression free survival No effect on overall survival Consensus, RT given immediately only if rapid disease progression is indicated
- 9. Supine, head to gantry Stabilisation – personalised neck shape and mask Localisation – head and neck baseboard CT or CT/MRI fusion
- 10. Vary depending on tumour location but include: ▪ Lens ▪ Uninvolved brain ▪ Pituatary glands ▪ Optic chiasm ▪ Optic nerves ▪ Brainstem ▪ Spinal cord
- 11. GTV/CTV/PTV and OAR contoured Conformal, IMRT as needed depending on tumour location Beam arrangement – considers OAR Upwards of three beams, weighting and wedges as required 45 – 66 Gy, most often 54/30/5
- 12. Anti-emetics prescribed as necessary Side effects monitored IMRT - Daily kV imaging Conformal – Weekly imaging
- 13. Hair loss Erythema Fatigue Change in taste Xerostima Headaches Worsening of seizures Nausea and vomiting
- 14. Cognitive impairment Changes in vision Stroke-like brain injury Effects on pituitary function (hormonal changes) Secondary cancers
- 15. Oligodendroglioma patients usually present with seizures Like all CNS tumours WHO classification over TNM staging Surgery is the best treatment approach Quite responsive to chemotherapy RT is not immediate but when patient becomes symptomatic Conformal or IMRT treatment
- 16. Abrey, L.E. , Childs, B.H., Paleologous, N et. al. 2006. “High dose chemotherapy with stem cell rescue as initial therapy for anaplastic oligodendroglioma: long term follow up”. Neuro Oncol. 8:183 Barrett, A. Dobbs, J. Morris, S. Roques, T. 2009. “Practical Radiotherapy Planning”. 4th edn, pp. 205-212, Hodder Arnold, London, United Kingdom. Cairncross JG, Wang M, Shaw EG, et.al. 2012. “Chemotherapy plus radiotherapy versus RT alone for patients with anaplastic oligodendroglioma: Long-term results of the RTOG 9402 phase III study”. J Clin Oncol 30s:2008b. Coons SW, Johnson PC, Scheithauer BW, Yates AJ, Pearl DK. 1997. “Improving diagnostic accuracy and interobserver concordance in the classification and grading of primary gliomas”. Cancer 79:1381–93. Daumas-Duport C, Varlet P, Tucker ML, Beuvon F, Cervera P, Chodkiewicz JP 1997. “Oligodendrogliomas. Part I: patterns of growth, histological diagnosis, clinical and imaging correlations: a study of 153 Cases”. J Neuro-Oncol 34:37–59. Desai SS, Paulino AC, Mai WY, Teh BS. 2006 “Radiation-induced moyamoya syndrome”. Int J Radiat Oncol Biol Phys 65:1222. Duffey P, Chari G, Cartlidge NE, Shaw PJ 1996. “Progressive deterioration of intellect and motor function occurring several decades after cranial irradiation. A new facet in the clinical spectrum of radiation encephalopathy”. Arch Neurol 53:814. Engelhard HH, Stelea A, Cochran EJ. 2002. “Oligodendroglioma: pathology and molecular biology”. Surg Neurol 57:111–7. Forsyth PA, Posner JB. Headaches in patients with brain tumors: a study of 111 patients. Neurology 1993; 43:1678. Gannett DE, Wisbeck WM, Silbergeld DL, Berger MS. 1994. “The role of postoperative irradiation in the treatment of oligodendroglioma”. Int J Radiat Oncol Biol Phys 30:567–73. Greenberg HS, Chandler WF, Sandler HM. 1999. “Brain Tumors”. New York: Oxford University Press. 189–200. Hussein MR, Baidas S. 2002. “Advances in diagnosis and management of oligodendrogliomas”. Expert Rev Anticancer Ther 2:520–8. Jenkinson MD, du Plessis DG, Smith TS, et al. 2006. “Histological growth patterns and genotype in oligodendroglial tumours: correlation with MRI features”. Brain 129:1884 Jukich PJ, McCarthy BJ, Surawicz TS, Freels S, Davis FG. Trends in incidence of primary brain tumors in the United States, 1985-1994. Neuro-Oncol 2001;3:141–51. Karim AB, Maat B, Hatlevoll R, et al. 1996. A randomized trial on dose-response in radiation therapy of low-grade cerebral glioma: European Organization for Research and Treatment of Cancer (EORTC) Study 22844. Int J Radiat Oncol Biol Phys 36:549. Keles GE, Lamborn KR, Berger MS. 2001. Low-grade hemispheric gliomas in adults: a critical review of extent of resection as a factor influencing outcome. J Neurosurg 95:735.
- 17. Lassman AB, Iwamoto FM, Cloughesy TF, et al. 2011. “International retrospective study of over 1000 adults with anaplastic oligodendroglial tumors”. Neuro Oncol 13:649. Lote K, Stenwig AE, Skullerud K, Hirschberg H. 1998. “Prevalence and prognostic significance of epilepsy in patients with gliomas”. Eur J Cancer 34:98. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK 2007. “World Health Organization Histological Classification of Tumours of the Central Nervous System”. Acta Neuropath 114: 1210 - 1216. Ludwig CL, Smith MT, Godfrey AD, Armbrustmacher VW. 1986. “A clinicopathological study of 323 patients with oligodendrogliomas”. Ann Neurol 19:15–21. Matthews, S., Succar, P., Jelinek, H., McParland, B., Buckland, M. & McLachlan, C. S. 2012. “Diagnosis of oligodendroglioma: Molecular and classical histological assessment in the twenty-first century”. Asia-Pacific Journal of Clinical Oncology, 8, 213-216 McGirt MJ, Chaichana KL, Attenello FJ, et al. 2008. “Extent of surgical resection is independently associated with survival in patients with hemispheric infiltrating low-grade gliomas”. Neurosurgery 63:700. Megyesi JF, Kachur E, Lee DH, et al. 2004. “Imaging correlates of molecular signatures in oligodendrogliomas”. Clin Cancer Res 10:4303. Olson JD, Riedel E, DeAngelis LM. Long-term outcome of low-grade oligodendroglioma and mixed glioma. Neurology 2000;54:1442–8. Paleologos NA. 2001. “Oligodendroglioma”. Curr Treatment Options Neurol 3:59–66. Reifenberger G, Kros JM, Burger PC, Louis DN, Collins VP.2000. “Oligodendroglioma”. In: Kleihues P, Cavenee WK, eds. Tumours of the Nervous System. Pathology and Genetics. Lyon: IARC Press, 56–61. Shah N, Pigott K, Bradford R. 1997. “Intradural drop metastases in oligodendrogliomas”. Clin Oncol R Coll Radiol 9:346–8. Shaw EG, Berkey B, Coons SW, et al.2008. “Recurrence following neurosurgeon-determined gross-total resection of adult supratentorial low-grade glioma: results of a prospective clinical trial”. J Neurosurg 109:835. Smith JS, Chang EF, Lamborn KR, et al. 2008. “Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas”. J Clin Oncol 26:1338. Squires RH Jr. 1989. “Intracranial tumors. Vomiting as a presenting sign. A gastroenterologist's perspective”. Clin Pediatr (Phila) 28:351. Taliansky-Aronov A, Bokstein F, Lavon I, Siegal T. 2006. “Temozolomide treatment for newly diagnosed anaplastic oligodendrogliomas: a clinical efficacy trial”. J Neurooncol 79:153. van den Bent MJ, Afra D, de Witte O, et al. 2005. “Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: the EORTC 22845 randomised trial”. Lancet 366:985. Van den Bent MJ, Kros JM, Heimans JJ, Pronk LC, van Groeningen CJ, Krouwer HGJ, et al. 1998. “Response rate and prognostic factors of recurrent oligodendroglioma treated with procarbazine, CCNU, and vincristine chemotherapy”. Neurology 51:1140–5.
Editor's Notes
- Oligodendrocytes are a type of glial cell found in the central nervous system (CNS) and can be seen in the image at the top right. Oligodendrogliomas are a CNS tumour which can be found anywhere that oligodendrocytes can be found. They are most commonly located in the cerebral hemispheres with 55% of all oligodendrogliomas located in the frontal lobe (Lessman, 1995;Ludwig, 1986). Other common locations include the temporal and parietal lobes (Ludwig, 1986). Only 4%, 3% and 1% are found in the occipital lobe, cerebellum and spinal cord respectively (Ludwig, 1986). Oligodendrogliomas are relatively slow growing (Matthews, 2012) and, whilst it is uncommon for them to spread outside of the CNS, such spread is more common than in other CNS tumours (Van den Bent, 1998; Shah, 1997).It is believed that this is due to the increased survival time of oligodendroglioma patients because of the slow growing nature of these tumours. Drop mets occur only 1 – 2% of the time (Van den Bent, 1998; Shah, 1997).
- Oligodendrogliomas are relatively rare accounting for 2 – 5% of brain tumours (Coons, 1997; Paeleologos, 2001; Daumas-Duport, 1997; Greenberg, 1999). It is estimated that oligodendrogliomas repesent 5 – 20% of all glial tumours (Jukich, 2001; Engelhard, 2002). The reason for such a large range is that in recent years the perceived incidence of oligodendrogliomas has increased. This is due to the introduction of MRI’s, which has increased the ability to detect these tumours and is also due to oligodendrogliomas previously being mis-diagnosed as astrocytomas (Jukich, 2001; Engelhard, 2002; Matthews, 2001). Oligodendrogliomas are most commonly found in 30 – 50 year olds and are rarely found in children. They occur almost equally in males and females and have no known aetiology aside from exposure to ionising radiaion.
- Oligodendroglioma present in the same manner as for all brain tumours. Symptoms can be generalised, as a result of the overall increased intracranial pressure, or focal, which arise from local pressure due to the growing tumour. The most common presenting symptom of oligodendroglioma is seizures (Lote, 1998). Patients may also develop these later if they don’t initially present with them. Like all other brain tumours oligodendroglioma patients also often present with headaches. These are indicitive of a brain tumour when accompanied by vomiting and nausea. Additionally, if they are worse at night, with change in body positioning eg standing to lying, or worse with coughing/sneezing etc. they can indicate a tumour (Forsyth, 1993). Syncope, a loss of consciousness due to increased intracranial pressure, and Cognitive dysfunction, such as memory problems or mood/personality changes can also occur as symptoms of Oligodendroglioma.
- The first step in diagnosing brain tumours is usually an MRI or CT scan. In the case of oligodendroglioma this is usually performed after a patient has presented to the doctor with seizures (Daumas – Duport, 1997; Olson, 2000). Although information from the MRI and/or CT could indicate Oligodendroglioma, imaging is mostly used to detect the location and spatial configuration of the tumour in order to plan for biopsy/surgery. Biopsies, usually by mean of surgical rescetion of the tumour, are the only way to get a definitive diagnosis (Jenkinson, 2006; Megyesi, 2004)
- Oligodendrogliomas are not staged using the TNM system but using the WHO guidelines (Louis, 2007). The WHO guidelines classify oligodendrogliomas into two tiers (Louis, 2007). The first tier, grade II tumours, are well differentiated. Their histology generally shows some atypical nuclei and low – moderate mitotic activity (Engelhard, 2002; Reifenberger, 2000). 77% of pure oligodendrogliomas are grade II. Grade three tumours are anaplastic oligodendrogliomas and account for 23% of pure oligodendrogliomas. Grade III oligodendrogliomas have moderate – high mitotic activity, noticable microvascular invasion, as shown by the arrows in the diagram, and necrosis (Engelhard, 2002; Reifenberger, 2000). It is worth noting that grade three tumours can occur initially or “morph” from grade II tumours.
- The standard treatment for Oligodendroglioma is surgical excision, with most studies suggesting full resection if possible (Kelles, 2001; Smith, 2008; Shaw, 2008; Hussein, 2002; McGirt, 2008). However, due to the infiltrating nature of this tumour full surgical excision is often not possible (Gannet, 1994; Shaw, 2008; Wallner, 1998). As such post operative Chemotherpy, Radiation therapy, or a combined approach is generally needed. Due to the slow growing nature of oligodendroglimoas studies suggest that radiotherapy treatment should be held off until the patient is symptomatic (Talinsky-Aronov, 2006; Abres, 2006; Karim, 1996). This will be discussed further in the next slide.
- There is currently a mixed opinion on the use of RT for Oligodendroglioma. One EORTC study conducted on 311 glioma patients administered immediate post- operative RT to some patients and delayed RT until symptoms appeared in the other patients. Upon reviewing these patients, on average 8 years later, it was found that, whilst giving immediate RT improved the progression free survival (5.4 years compared to 3.7 years for delayed RT) there was no overall survival benefit from the immediate radiation (van den Bent, 2005). Because of this study and many like it most often RT is delayed until symptoms appear. Immeadiate RT is given only in the cases where rapid disease progression is indicated (Cairncross, 2012; Karim, 1996).
- Oligodendroglioma treatment is simulated and planned as for any other glioma treatment. Patients are supine and are stabilised using a personalised neck shape and mask of some sort. They are located on the bed using the equipment such as a head and neck baseboard. A CT scan is taken and this is sometimes fused with an MRI to obtain greater tumour delineation.
- As with any head and neck cancer there are many organs at risk which need to considered when planning radiation therapy for Oligodendroglioma such as the lenses and spinal cord. Organs at risk vary depending on the tumour location (Barrett, 2009).
- Where the tumour was not fully excised a GTV is marked as well as a CTV and these are expanded to obtain the PTV. OAR, which are tumour site dependent, are also contoured. The treatment is then planned, with consideration to tumour loction. Both conformal planning and, where OAR are in close proximity, IMRT should be considered. In either situation beams should be placed so as to avoid dose to OAR and maximise dose to the PTV (Barrett, 2009). Generally there are three or more beamsn, angled to avoid dose to OAR (Barrett, 2009). 54Gy in 30 fractions is a typical dose but can vary.
- Patients should be monitored in a daily basis for side effects. Dr’s should be informed in dexamthasone or anti-emitcs are required and the patient is not yet taking them. Image verification should be completed for all treatments. For the highly conformal IMRT plan treatment should be verified with daily kV imaging. Online corrections made and verified, by re-imaging before treatment. For conformal plans, where dose gradients are not as steep, weekly imaging, with offline corrections are adequate to ensure treatment is delivered accurately.
- As with any radiation therapy there are many expected side effects for treating oligodendroglioma with RT (Squires, 1989). These are the potential acute side effects, obviously the occurrence of these depends on the tumour site. Some form of hair loss, fatigues and erythema is expected with all patients (Squires, 1989). In some cases the patients seizures actually worsen briefly before becoming increasingly better. Most patients hair will grow back of its own accord but, should it not, wigs and other hair accessories can be suggested. Erythema should be managed with good skin care in consultation with the nursing staff. Oral symptoms can be managed with products such as biotene and nausea and vomitting can be managed with antiemetics.
- There are also late effects from RT for Oligodendroglioma such as Cognitive impairment Changes in vision Stroke-like brain injury Effects on pituitary function (hormonal changes) Secondary cancers (Olsson, 2000; Duffey, 1996; Desai, 2006).
- Oligodendroglioma patients usually present with seizures Like all CNS tumours WHO classification over TNM staging Surgery is the best treatment approach Quite responsive to chemotherapy RT is not immediate but when patient becomes symptomatic Conformal or IMRT treatment