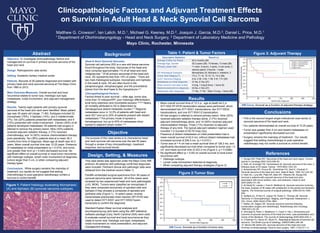
1. Figure 2:Tumor Size
KM Curve. Survival as a function of tumor size.
Clinicopathologic Factors and Adjuvant Treatment Effects
on Survival in Adult Head & Neck Synovial Cell Sarcoma
2013 Mayo Foundation for Medical Education and Research
Matthew G. Crowson1, Ian Lalich, M.D.1, Michael G. Keeney, M.D.2, Joaquin J. Garcia, M.D.2, Daniel L. Price, M.D.1
1 Department of Otorhinolaryngology - Head and Neck Surgery, 2 Department of Laboratory Medicine and Pathology
Mayo Clinic, Rochester, Minnesota
• This is the second largest single institutional case series of
synovial sarcoma of the head and neck.
• Our patients demonstrated an overall survival of 12.25 years.
• Tumor size greater than 4 cm and distant metastases on
presentation significantly decreased survival.
• Surgery remains the mainstay of treatment . Our results
suggest that adding chemotherapy to post-operative
radiotherapy may not confer a survival or control benefit.
Conclusions
1. Sturgis EM, Potter BO. Sarcomas of the head and neck region. Current
opinion in oncology.2003;15(3):239–52.
2. Roth JA, Enzinger FM, Tannenbaum M. Synovial sarcoma of the neck: a
followup study of 24 cases. Cancer. 1975;35(4):1243–53.
3. Bukachevsky RP, Pincus RL, Shechtman FG, Sarti E, Chodosh P.
Synovial sarcoma of the head and neck. Head & Neck. 1992;14(1):44–48.
4. Harb WJ, Luna MA, Patel SR, Ballo MT, Roberts DB, Sturgis EM.
Survival in patients with synovial sarcoma of the head and neck:
association with tumor location, size, and extension. Head & neck.
2007;29(8):731–40.
5. Al-Daraji W, Lasota J, Foss R, Miettinen M. Synovial sarcoma involving
the head: analysis of 36 cases with predilection to the parotid and temporal
regions. The American journal of surgical pathology. 2009;33(10):1494–
503.
6. Spillane AJ, A’Hern R, Judson IR, Fisher C, Thomas JM. Synovial
Sarcoma: A Clinicopathologic, Staging, and Prognostic Assessment. J.
Clin. Oncol. 2000;18(22):3794–3803..
7. Mullen JR, Zagars GK. Synovial sarcoma outcome following
conservation surgery and radiotherapy. Radiotherapy and Oncology.
1994;33(1):23–30.
8. Simunjak B, Petric V, Bedekovic V, Cupić H, Hat J. Dimensions and
outcome of synovial sarcoma of the head and neck: case presentation and
review of the literature. The Journal of otolaryngology.2005;34(6):420–3.
9. O’Sullivan PJ, Harris AC, Munk PL. Radiological features of synovial cell
sarcoma. The British journal of radiology. 2008;81(964):346–56.
10. Moore DM, Berke GS. Synovial sarcoma of the head and neck.
Archives of otolaryngology--head & neck surgery. 1987;113(3):311–3.
References
Objective. To investigate clinicopathologic factors and
management on survival in primary synovial sarcoma of the
head and neck.
Design. Retrospective case series.
Setting. Academic tertiary medical center.
Patients. Records of 28 patients diagnosed and treated with
primary head and neck synovial sarcoma at The Mayo Clinic
from 1960 to 2012.
Main Outcome Measures. Overall survival and local
recurrence related to tumor size, histologic sub-type,
metastases, nodal involvement, and adjuvant management
strategy.
Results. Twenty-eight patients with primary synovial
sarcoma of the head and neck were identified. Mean patient
age was 35 years old (range, 11-80). Subtypes included 22
monophasic (79%), 4 biphasic (14%), and 2 indeterminate
(7%). Six (22%) patients presented with metastases, and 4
(15%) presented with nodal involvement. Eleven (39%) of all
patients developed metastases. All patients had surgery in
attempt to remove the primary lesion. Nine (32%) patients
received adjuvant radiation therapy, 2 (7%) received
chemotherapy, and 14 (50%) receive chemoradiation therapy
post-operatively. Ten (36%) patients died at a mean 38.3
months from time of diagnosis. Mean age at death was 44.2
years. Mean overall survival time was 12.25 years. Presence
of metastases on initial presentation (p = 0.015), and tumor
size greater than 4cm (p = 0.040) decreased survival. No
significant effect on overall survival or local tumor recurrence
with histologic subtype, lymph node involvement at diagnosis,
tumors larger than 5 cm, or when comparing adjuvant
therapy types.
Conclusions. While surgery remains the mainstay of
treatment, our results do not suggest that adding
chemotherapy to post-operative radiotherapy confers a
survival or control benefit.
Abstract
Head & Neck Synovial Sarcoma:
Synovial cell sarcoma (SS) is a rare soft tissue sarcoma
found throughout the body. Sarcomas of the head and
neck comprise approximately 1% of all head and neck
malignancies.1 Of all primary sarcomas of the head and
neck, SS represents less than 10% of cases.1 There are
two main histological subtypes: monophasic and biphasic.
In the head & neck, SS are often found in the
parapharyngeal, retropharyngeal, and the prevertebral
planes from the skull base to the hypopharynx.2,3
Clincopathological Factors:
Factors linked to poor survival – older age, tumor size,
more than 10 mitoses/HPF, poor histologic differentiation,
local bony extension and incomplete excision.3,4,5,6 Nearly
all mortality attributed to SS is determined by
hematogenous distant metastatic burden.4,7 Regional
metastases occur in 12.5% of patients with head and
neck SS,8 and up to 25% of patients present with distant
metastases.9 The primary mode of spread is
hematogenous, but up to 20% of metastases show
spread to adjacent lymph nodes.2,10
Background
• Mean overall survival time of 12.3 yr., age at death 44.2 yr.
• SYT-SSX RT-PCR translocation assays were performed, which
demonstrated two SYT-SSX1 translocations, two SYT-SSX2
translocations, and one SYT-SSX1/2 translocation.
• All had surgery in attempt to remove primary lesion. Nine (32%)
received adjuvant radiation therapy alone, 2 (7%) received
adjuvant chemotherapy alone, and 14 (50%) received adjuvant
chemoradiation therapy. Three (11%) received no adjuvant
therapy of any kind. The typical adjuvant radiation regimen used
included 1-2 courses of 50-70 Gray (Gy).
• Presence of distant metastases on initial presentation had a
mean overall survival of 42.0 mo, without distant metastases had
increased survival of 206.5 mo. (p = 0.0151).
• Tumor size of > 4 cm had a mean survival time of 128.2 mo, and
significantly decreased survival when compared to tumor size < 4
cm and mean survival time of 223.2 mo (Figure 2, p = 0.0396).
• No significant effect (p > 0.05) on overall survival or local tumor
recurrence with:
• Histologic subtype.
• Lymph node involvement detected at diagnosis.
• When comparing adjuvant therapy strategies (Figure 3).
Results
The purpose of this case series is to characterize head
and neck synovial cell sarcoma over the last 50 years
through a review of key clinicopathologic, treatment
response, and survival trends.
Objective
This case series was approved under the Mayo Clinic IRB
protocol. All patients with pathology-confirmed diagnoses
were included. Pertinent clinical and pathologic data were
obtained from the medical record (Table 1).
Paraffin-embedded surgical specimens from 36 cases of
synovial sarcoma were retrieved. All of the cases were
reviewed by two experienced head and neck pathologists
(JJG, MGK). Tumors were classified as monophasic if
they were composed exclusively of spindled cells and
biphasic if they showed a composite of spindled and
epithelial cells (Figure 1). In select cases, reverse
transcriptase-polymerase chain reaction (RT-PCR) was
used to detect SYT-SSX1 and SYT-SSX2 fusion
transcripts to confirm the diagnosis.
Standard Kaplan-Meier survival analyses and
accompanying log-rank tests using the JMP statistical
software package (Cary, North Carolina USA) were used
to evaluate overall survival and local recurrence as they
relate to tumor size, histologic sub-type, metastases,
nodal involvement on initial presentation, and adjuvant
management strategy.
Design, Setting, & Measures
Table 1: Patient & Tumor Factors Figure 3: Adjuvant Therapy
KM Curve. Survival as a function of adjuvant therapy strategy.
Descriptive Statistics Result (n)
Average Follow-Up Period 83.4 months (26)
Average Age; Gender 35.3 years (28); 15 female, 13 male (28)
Primary Lesion Site 11 neck, 5 larynx, 4 spine, 3 oral cavity, 2
salivary gland, 2 thyroid, 1 scalp
SS Histological Subtypes Monophasic 22, Biphasic 4, Indeterm. 2
Tumor Size Staging (T) TX 2, T1 16, T2 10, T3, T4 0 (28)
AJCC Sarcoma Staging 9 IA, 2 IB, 3 IIA, 1 IIB, 5 III, 7 IV (28)
Metastases on initial diagnosis 21 No, 6 Yes (27)
Most common met sites (initial) 4 lung, 1 lung & bone, 1 bone (6)
Nodal involvement on diagnosis 23 No, 4 Yes (27)
Metastases after diagnoses 11 Yes, 17 No . Sites 10 lung, 1 bone (28)
Figure 1: Patient histology illustrating Monophasic
(A) and biphasic (B) synovial sarcoma subtypes.