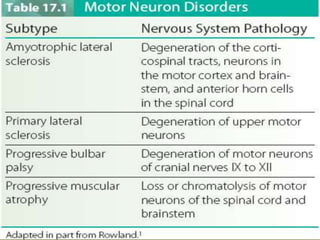
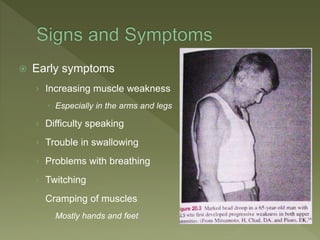
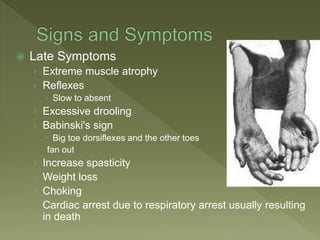
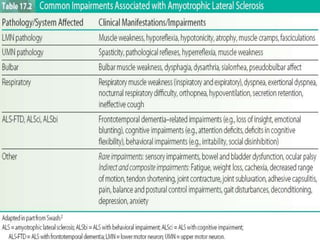
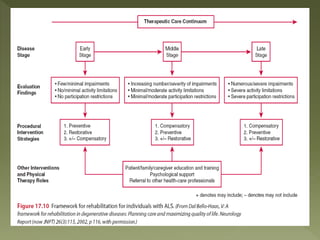
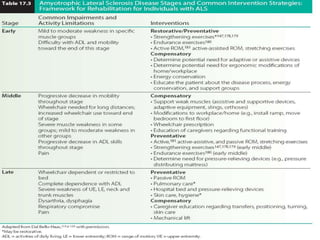
This document discusses amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig's disease. It is a progressive neurodegenerative disease that affects motor neurons in the brain and spinal cord, resulting in muscle weakness, paralysis, and eventually death, usually within 3 to 5 years of diagnosis. The cause is generally unknown but may involve genetic mutations, free radicals, glutamate toxicity, or an autoimmune response. Symptoms start with muscle weakness and progress to include difficulty speaking, swallowing, and breathing. There is no cure and treatment aims to manage symptoms and improve quality of life.