Recommended

More Related Content
What's hot
What's hot (10)
Similar to AMCHP_Poster_Final
Similar to AMCHP_Poster_Final (20)
AMCHP_Poster_Final
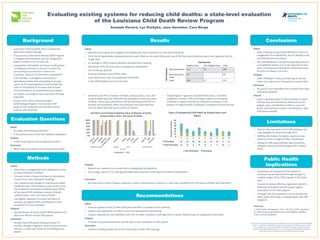
- 1. Conclusions Public Health Implications Methods Background Results Evaluation Questions Limitations Recommendations Evaluating existing systems for reducing child deaths: a state-level evaluation of the Louisiana Child Death Review Program Amanda Pereira, Lyn Kieltyka, Jane Herwehe, Cara Bergo • Louisiana’s child mortality rate is consistently above the na5onal average • The Louisiana Child Death Review (CDR) Program is charged with reviewing cases of unexpected death in children 0 to 14 years old • Unexpected child deaths are those resul5ng from “undiagnosed disease, or trauma in which the surrounding circumstances of which are suspicious, obscure, or otherwise unexplained”1 • A 25-‐member, mul5-‐agency state panel is legisla5vely tasked with comple5ng an annual report for the state legislature that reviews the state of child deaths in Louisiana and includes recommenda5ons for preven5ng future deaths • As of 2015, the program has never been formally evaluated • As part of the 2015 Graduate Student Epidemiology Program, the Louisiana CDR program was evaluated via state-‐level inputs, outputs, and outcomes Inputs • Are state CDR mee5ngs effec5ve? • Is the performance of the CDR database adequate? Outputs • Is CDR producing an annual legisla5ve report? Outcomes • What state-‐level ac5ons have resulted from CDR? Inputs • Administer an engagement and sa5sfac5on survey to state CDR panel members • Compare roster of panel members to aVendance records from state CDR panel mee5ngs • Use a determinis5c linkage of Vital Records death cer5ficates with CDR database cases to determine the sensi5vity and posi5ve predic5ve value (PPV) of the overall CDR database, manner of death, autopsy status, race, and cause of death • Use logis5c regression to assess the effect of turnover of regional MCH coordinators on the propor5on of cases reviewed Outputs • Review Bureau of Family Health (BFH) website and electronic files for annual CDR reports Outcomes • Review state CDR panel mee5ng minutes for prac5ce changes, programs, system improvements, policies, or state laws aimed at preven5ng future deaths Inputs • State mee5ngs are generally effec5ve in terms of engagement and sa5sfac5on, but are lacking in full membership and aVendance • The CDR database is not performing adequately as a surveillance system as it is not capturing all true cases of unexpected child death. Abstracted cases are also not always true cases Outputs • CDR is fulfilling it’s duty of producing an annual report, but reports are not based on current data Outcomes • No ac5ons were iden5fied that resulted from state CDR panel ac5vi5es Overall • Areas in greatest need of improvement are panel membership and aVendance, abstrac5on of all eligible cases, classifica5on of SIDS as cause of death, and tracking of ac5ons resul5ng from state CDR panel ac5vi5es. • Data for the evalua5on of the CDR database was only available for deaths through 2013 • Staffing informa5on for logis5c regression was based on recall of regional MCH coordinators • Review of CDR panel ac5vi5es were limited to available mee5ng minutes (August 2011-‐March 2015) • Surveillance of unexpected child deaths in Louisiana can be improved through changes in mul5ple stages of the CDR program at the state-‐ level • In order to remain effec5ve, legisla5on aimed at reducing child deaths should require regular evalua5ons of the CDR program • Findings from this evalua5on can be shared with other states that hope to evaluate their own CDR programs Reference: 1. Child Death Inves5ga5on, Pub. L. No. 40, § 2019. Available at: hVps://legis.la.gov/Legis/Law.aspx?d=98002. Updated 1999. Accessed 6/8/2015. This project was supported in part by the Health Resources and Services Administra5on (HRSA) of the U.S. Department of Health and Human Services (HHS) Title V MCH Block Grant award. This informa5on or content and conclusions are those of the author and should not be construed as the official posi5on or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government. (or any other disclaimer needed) Inputs • Members were generally engaged and sa5sfied with their experience on the state CDR panel • 20 of the 25 legisla5vely mandated posi5ons were filled on the state CDR panel; two of the five vacant posi5ons were from agencies that no longer exist • An average of 39% of panel members aVended each mee5ng • Sensi5vity= 67%; All true cases of unexpected child deaths are not being captured • Posi5ve Predic5ve Value (PPV)= 84%; some abstracted cases of unexpected child death in the CDR database are not true cases Vital Records Eligible Cases Non-‐eligible Cases Total CDR Database Abstracted Cases 141 27 168 Non-‐abstracted Cases 69 -‐-‐ 69 Total 210 27 137 • Sensi5vity and PPV of manner of death, autopsy status, race, and cause of death was over 90% with the excep5on of SIDS as a cause of death, which had a sensi5vity of 29.4% (sensi5vity and PPV for suicides and homicides; other and unknown race; and unknown cause of death was low due to small cell counts) Outputs • Reports are created on an annual basis as designated by legisla5on • On average, there is a 3.5 year gap between data covered in CDR reports and date of publica5on. Outcomes • No state-‐level prac5ce changes, programs, system improvements, policies, or state laws resul5ng from CDR panel ac5vi5es were iden5fied • Simple logis5c regression indicated there was a 3.58 (95% confidence interval: 2.05-‐6.25) higher odds of a case being reviewed in regions that did not experience turnover in the posi5on of regional MCH coordinator compared to those that did Inputs • Keep an updated roster of state CDR panel members to review at each mee5ng • Update state legisla5on to reflect current and appropriate membership • Using an opera5onal case defini5on with ICD-‐10 codes, establish a new algorithm to beVer iden5fy cases of unexpected child death Outputs • Consider using provisional vital records data in the comple5on of CDR reports Outcomes • Employ a tracking system for ac5ons discussed at state CDR mee5ngs 0%# 20%# 40%# 60%# 80%# 100%# Natural# Accidental#Suicide# Hom icide# Undeterm ined# Autopsy# W hite## Black#Other# Unknow n# External# SIDS# Unknow n# SensiGvity#and#PosiGve#PredicGve#Value#of#Manner#of#Death,# Autopsy#Status,#Race,#and#Cause#of#Death# SensiGvity# PPV# Manner of Death Autopsy Race Cause of Death Variable 1" 2" 3" 4" 5" 6" 7" 8" 9" Reviewed" 27" 15" 16" 24" 11" 12" 23" 0" 17" Not"Reviewed" 21" 13" 4" 9" 8" 3" 7" 19" 1" 0" 10" 20" 30" 40" 50" 60" Number"of"Cases" Cases"of"Unexpected"Child"Death"by"Review"Status"and" Region"" ! Not"Reviewed" Reviewed"