
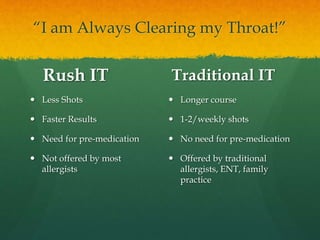


This document summarizes information from a presentation on allergies given by Dr. Summit Shah. It discusses common allergy symptoms, the mechanisms of allergic reactions and anaphylaxis, treatments including avoidance, medications, and immunotherapy, and myths about allergies. Rush immunotherapy provides faster results than traditional immunotherapy but requires pre-medication, while traditional immunotherapy involves longer treatment with weekly shots but no pre-medication. Food is a leading cause of anaphylaxis, and accidental exposures are common. Proper and immediate epinephrine administration is important for treating anaphylactic reactions.





























































































