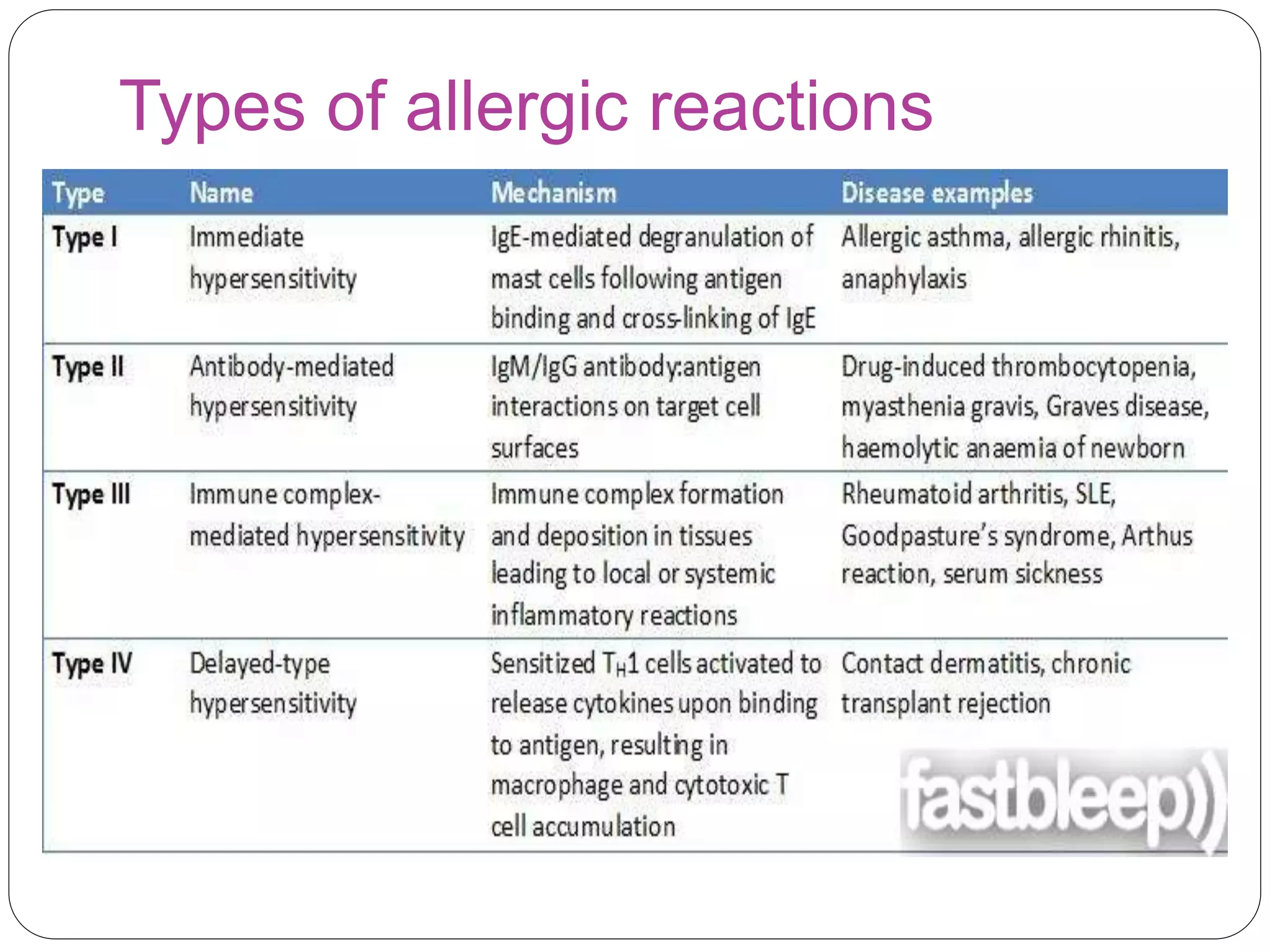
Allergic disorders are common in children, affecting 15-30% globally. Allergies are caused by an inappropriate immune response to substances called allergens. Common allergic disorders in children include allergic rhinitis, atopic dermatitis, urticaria, insect bites, food allergy, and anaphylaxis. Allergic reactions involve the release of mediators like histamine from immune cells. Treatment focuses on avoidance of triggers, antihistamines, and management of symptoms.