1. ⏐ FIELD ACTION REPORT ⏐
Supplement 3, 2015, Vol 105, No. S3 | American Journal of Public Health Fawcett et al. | Peer Reviewed | Field Action Report | S433
Participatory Evaluation of a Community Mobilization
Effort to Enroll Wyandotte County, Kansas, Residents
Through the Affordable Care Act
| Stephen B. Fawcett, PhD, Charles E. Sepers, BS, Jerry Jones, BA, Lucia Jones, RN, BSN, CEN, and Wesley McKain, BA
Successful implementation of the Affordable Care Act (ACA)
depends on the capacity of local communities to mobilize for
action. Yet the literature offers few systematic investigations of
what communities are doing to ensure support for enrollment.
In this empirical case study, we report implementation and
outcomes of Enroll Wyandotte, a community mobilization effort
to facilitate enrollment through the ACA in Wyandotte County,
Kansas. We describe mobilization activities during the first
round of open enrollment in coverage under the ACA (October
1, 2013–March 31, 2014), including the unfolding of commu-
nity and organizational changes (e.g., new enrollment sites) and
services provided to assist enrollment over time. The findings
show an association between implementation measures and
newly created accounts under the ACA (the primary outcome).
(Am J Public Health. 2015;105:S433–S437. doi:10.2105/
AJPH.2014.302505)
accounts under the ACA (the
primary outcome). We describe
how participatory research meth-
ods were used to systematically
reflect on progress and use the
data to make adjustments.
COMMUNITY
MOBILIZATION FOR
ENROLLMENT
Wyandotte County (Kansas
City; population=160384)6
is
an area with low incomes and
high disparities in health out-
comes; it ranks 96 of 98 in the
county health rankings for the
state of Kansas.7
This culturally
diverse community has limited
access to health care services,
and its residents are 24.4%
African American and 26.9%
Latino.8
Enroll Wyandotte has the mis-
sion of ensuring access to health
care for all Wyandotte County
residents by enabling enrollment
in health insurance. To support
enrollment through the ACA,
Enroll Wyandotte engaged mul-
tiple partners from different sec-
tors; for instance, governmental
health organizations (Wyandotte
KEY FINDINGS
Community mobilization resulted in expanded access to places for en-
rollment and people to support residents in enrolling for health insur-
ance.
Funding support made it possible to hire staff who helped to coordinate
the work in creating these new settings and in recruiting and supporting
volunteers.
Collaboration with an existing coalition, the Latino Health for All Coali-
tion, helped engage community partners in planning, implementation,
and participatory evaluation.
MINORITY POPULATIONS
experience the greatest dis-
parities in health and associated
access to health care.1,2
The Af-
fordable Care Act (ACA)3
is land-
mark federal legislation intended
to increase health care access
among those who need it.4
State-
level supports for access vary
enormously; some states have
attempted to erect barriers to
impede enrollment.5
Thus, ensur-
ing enrollment through the ACA
is typically a local matter requir-
ing community mobilization and
partnerships.
In this empirical case study,
we report implementation and
outcomes of Enroll Wyandotte, a
community mobilization effort to
facilitate enrollment through the
ACA (October 1, 2013–March
31, 2014) in Wyandotte County,
Kansas. We describe mobiliza-
tion activities, including commu-
nity and organizational changes
(e.g., new enrollment sites,
expanded hours for enrollment)
and services provided (e.g., in-
stances of enrollment assistance).
The report provides data on the
association between implementa-
tion measures and newly created
2. ⏐ FIELD ACTION REPORT ⏐
American Journal of Public Health | Supplement 3, 2015, Vol 105, No. S3S434 | Field Action Report | Peer Reviewed | Fawcett et al.
the ACA and associated access
to needed health care, especially
among those experiencing health
disparities. Community partners
identified several key indicators
of success: (1) community and
organizational changes (i.e., new
or modified programs, policies,
or practices to facilitate enroll-
ment through the ACA, such as
expanded enrollment hours at
the health department, new sites
at local public libraries, and com-
munity organizations), (2) services
provided (e.g., media communica-
tions to promote awareness, direct
assistance in enrollment sites),
and (3) created accounts (the total
number of family accounts cre-
ated within the ACA Web site at
3 enrollment sites).
Table 1 shows the monitor-
ing and evaluation system used
with Enroll Wyandotte, including
evaluation questions, indicators,
and type of measurement.
Documenting Implementation
and Outcomes
The Work Group for Com-
munity Health and Development
team designed an online docu-
mentation and support system9
that included prompts and sup-
ports to (1) capture instances of
community and organizational
changes and services provided
(i.e., what was done when and
by whom toward what goal),
(2) code by type of activity (i.e.,
using definitions of community
and organizational change and
services provided), (3) charac-
terize the activity (e.g., by goal,
strategy used, sector in which
implemented), and (4) communi-
cate progress (e.g., graphs of the
unfolding of community and or-
ganizational changes over time).
The Sidebar shows illustrative
community and organizational
changes (i.e., new or modified
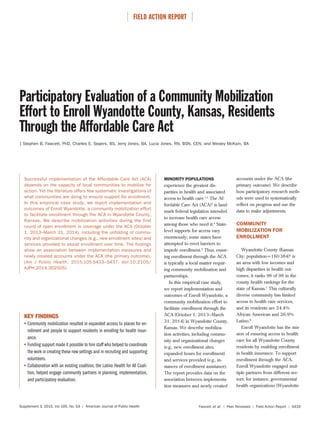
Note. CAC=Certified Application Assistors; CC=community change; HCF=Health Care Foundation of Greater Kansas City; KC=Kansas City;
KU=University of Kansas; OC=organizational change; SP=services provided. In a cumulative chart, each new activity is added to all prior
activities. CC/OC × created accounts: r(16)=0.638; P=.004. Enrollment SP × created accounts: r(16)=0.581; P=.011.
FIGURE 1—Cumulative number of community and organizational changes, services provided, and created
accounts over time for Enroll Wyandotte during the first open enrollment period for the Affordable Care
Act: Wyandotte County, Kansas, October 1, 2013–March 31, 2014.
County Health Department),
public institutions (e.g., librar-
ies), hospitals and health care
organizations (e.g., safety net
clinics), community and cultural
organizations (e.g., El Centro),
universities (e.g., University of
Kansas), and community health
coalitions (e.g., Latino Health for
All Coalition).
Enroll Wyandotte used a com-
munity mobilization approach to
increase awareness, accessible
settings, and human resources
to make enrollment through
the ACA easier for residents.
The Sidebar outlines the core
intervention components and
elements of this strategy and il-
lustrative activities.
PARTICIPATORY
EVALUATION OF ENROLL
WYANDOTTE
This participatory evalua-
tion engaged both community
partners—staff and leadership of
Enroll Wyandotte (J.J., L.J., and
W.M.)—and a research partner,
the Work Group for Community
Health and Development at the
University of Kansas (S.B.F. and
C.E.S.). Community and research
partners worked together to
identify key evaluation questions
and related indicators to support
participatory sensemaking and
program improvement.
Identifying Indicators of
Success
The vision for Enroll Wyan-
dotte was ensuring conditions for
widespread enrollment through
3. ⏐ FIELD ACTION REPORT ⏐
Supplement 3, 2015, Vol 105, No. S3 | American Journal of Public Health Fawcett et al. | Peer Reviewed | Field Action Report | S435
Description of Enroll Wyandotte Intervention Components and Elements and Illustrative Activities: Wyandotte County/Kansas City, Kansas
Components Intervention Elements With Illustrative Community and Organizational Changes and Services Provided Type of Activity
Providing information and
enhancing skills
Provided one-on-one education through the walk-in enrollment center. Services provided
Provided ACA enrollment information to community outreach partners (e.g., community development organizations,
neighborhood associations).
Services provided
Provided ACA education materials through local health fairs and other community settings (e.g., elementary schools, churches,
government buildings).
Services provided
Provided inbound and outbound education through the enrollment center. Services provided
Community partners (e.g., neighborhood associations, charities, university medical centers) in collaboration with Enroll
Wyandotte provided informal education sessions and distributed education materials within their communities.
Services provided
Conducted a social marketing campaign that included radio advertisements of education and enrollment events, radio
interviews, and print-media coverage.
Services provided
Conducted a door-to-door education referral campaign (Canvas Kansas City) to identify eligible community residents. Services provided
Enroll Wyandotte, in partnership with the Health Care Foundation of Greater Kansas City, called resident referrals identified
from the door-to-door campaign.
Community and organizational
change
Modifying access, barriers,
exposures, and opportunities
Provided one-on-one enrollment assistance through the walk-in enrollment center. Services provided
Provided one-on-one enrollment assistance with community residents through satellite enrollment sites (e.g., libraries, charity
organizations).
Services provided
Provided inbound enrollment assistance through the enrollment center. Services provided
Conducted community enrollment events in collaboration with community partners (e.g., recreation facilities, charity
organizations).
Services provided
Enhancing services and
support
Hired a full-time navigator/project coordinator. Community and organizational
change
Trained a workforce of university volunteers as certified application assistors. Volunteers engaged
Expanded the enrollment center from 1 to 5 d/wk. Organizational change
Modifying policies and
broader systems
Established collaborative partnerships with community organizations (e.g., safety net clinics, public libraries, volunteer
groups).
Community and organizational
change
Established a walk-in enrollment center in collaboration with the Wyandotte County Health Department. Community and organizational
change
Established the Wyandotte County Health Department as a certified US Department of Health and Human Services training
center for enrollment assistors.
Community and organizational
change
Provided testimony to senate committees: Enroll Wyandotte staff provided testimony to state legislators in opposition of SB
362, a bill that would have required mandatory background checks on navigators and other application assistors at the
expense of $300 each.
Community action
Note. ACA=Affordable Care Act.
4. ⏐ FIELD ACTION REPORT ⏐
American Journal of Public Health | Supplement 3, 2015, Vol 105, No. S3S436 | Field Action Report | Peer Reviewed | Fawcett et al.
programs, policies, and practices)
and services provided (e.g., in-
stances of enrollment assistance)
associated with implementation
of the intervention elements of
Enroll Wyandotte.
Figure 1 displays the cumula-
tive number of community and
organizational changes, services
provided, and created accounts
over time for Enroll Wyandotte
during the first enrollment period
under the ACA. The results show
a gradual unfolding of commu-
nity and organizational changes
(n=9) and services provided
(n=73) to support enrollment
of Wyandotte County residents
through the ACA. This was as-
sociated with a corresponding
increase in the outcome indicator
of created accounts (n=539). A
statistically significant association
was found between created ac-
counts and community and orga-
nizational changes and between
created accounts and enrollment
services provided (Figure 1).
Evaluation Question Indicators Measurement Frequency Person Responsible Related Activities
Goal 1: Engage in community mobilization and change efforts to enable access to health insurance
Is the initiative bringing
about changes in
communities and
systems related to the
mission?
No. and type of
community and
organizational
change
Project records Summarized monthly in online
documentation and support
system
Project documenters Quarterly sensemaking
and reports to
funders
Documented in online
documentation and support
system (community and
organizational change)
Goal 2: Ensure information and support services for those enrolling in health insurance
Are we providing
information and support
services to uninsured
residents?
No. of services
provided to
enrollees
Project records Summarized monthly in online
documentation and support
system
Project documenters Quarterly sensemaking
and reports to
funders
Documented in online
documentation and support
system (services provided)
Goal 3: Increase enrollment in health insurance among residents of Wyandotte County
Is there an increase in
enrollment applications
completed?
No. of enrollment
applications
completed
Project records Summarized in online
documentation and support
system after each available
measurement (e.g., quarterly,
annual)
Project documenters Biannual sensemaking
and reports to
funders
Documented in online
documentation and support
system (indicators database)
Participatory Sensemaking
and Adjustments
The online documentation and
support system also supported
participatory sensemaking9
by
pairing graphs of activities and
outcomes with reflection ques-
tions:
1. What are we seeing? (e.g.,
the graph shows a marked
increase in services provided
beginning in late December
2013)
2. What does it mean? (e.g., this
increase was associated with
hiring an overall coordinator
and site coordinators that was
made possible by community
foundation funding and col-
laboration with community
partners)
3. What are the implications
for adjustment? (e.g., to in-
crease enrollment, we need
to expand enrollment sites
and engage more volunteers
to provide support within
them)
SUMMARY
This empirical case study was
one of the first systematic investi-
gations of the effects of commu-
nity mobilization to enroll resi-
dents in health insurance
through the ACA. Community
and research partners used data
and shared sensemaking to iden-
tify features that appear to have
supported implementation and
outcomes. Population health and
health equity require condi-
tions—such as universal access to
health care—that reduce the dif-
ferential vulnerabilities and
health consequences that pro-
duce health disparities.10
About the Authors
Stephen B. Fawcett and Charles E. Sepers
are with the Work Group for Community
Health and Development, a World Health
Organization Collaborating Centre, Uni-
versity of Kansas, Lawrence. Jerry Jones
and Lucia Jones are with Enroll Wyan-
dotte and its parent organization, the
Community Health Council of Wyandotte
County, Kansas City, KS. Wesley McKain
is with Healthy Communities Wyandotte,
Kansas City.
Correspondence should be sent to
Stephen B. Fawcett, PhD, Work Group
for Community Health and Develop-
ment, 1000 Sunnyside Ave, 4082 Dole
Center, University of Kansas, Lawrence,
KS 66045 (e-mail: sfawcett@ku.edu)
or Jerry Jones, BA, Community Health
Council, 755 Minnesota Ave, Kansas
City, KS 66101 (e-mail: jjones@wy-
cohealth.com). Reprints can be ordered
at http://www.ajph.org by clicking the
“Reprints” link.
This article was accepted November
26, 2014.
Contributors
S.B. Fawcett and C.E. Sepers originated
and drafted the article. All authors re-
viewed and revised drafts of the article.
Acknowledgments
Implementation and documentation of
Enroll Wyandotte was supported by
grants from the REACH Healthcare
Foundation and Health Care Foundation
of Greater Kansas City. Participatory
research was supported by the National
Institute on Minority Health and Health
Disparities (NIMHD; grant NIH51190)
to the Work Group for Community
Health and Development, University of
Kansas. This NIMHD grant supported
participatory research with the Latino
TABLE 1—Monitoring and Evaluation System Used With the Enroll Wyandotte Effort: Wyandotte County, Kansas, August 2013–March 2014
5. ⏐ FIELD ACTION REPORT ⏐
Supplement 3, 2015, Vol 105, No. S3 | American Journal of Public Health Fawcett et al. | Peer Reviewed | Field Action Report | S437
Health for All Coalition, a collaborative
partner of Enroll Wyandotte.
The authors wish to acknowledge
the collaboration of the many com-
munity partners who made the work
of Enroll Wyandotte possible. We also
appreciate the research support of Vicki
Collie-Akers, our colleague at the Work
Group for Community Health and De-
velopment.
Human Participant Protection
The study, a part of a broader partici-
patory research study of the Latino
Health for All Coalition, was reviewed
and approved by the Human Subjects
Committee at the University of Kansas.
Human participants were not the focus
of the research conducted. The unit of
analysis was organizational rather than
individual level. No personal identi-
fiers were collected. Individuals in this
study faced no substantial risk.
References
1. Frieden TR, Centers for Disease
Control and Prevention. Forward: CDC
health disparities and inequalities report
- United States, 2011. MMWR Surveill
Summ. 2011;60(suppl):1–2.
2. Schiller JS, Ward BW, Freeman G,
Peregoy JA. Early release of selected esti-
mates based on data from the 2012 Na-
tional Health Interview Survey. National
Center for Health Statistics. June 2013.
Available at: http://www.cdc.gov/nchs/
nhis.htm. Accessed June 24, 2014.
3. The Patient Protection and Afford-
able Care Act, Pub. L. No. 111-148,
124 Stat. 855 (March 2010).
4. Fielding JE, Teutsch S, Koh H. Health
reform and healthy people initiative.
Am J Public Health. 2012;102(1):30–
33.
5. Cauchi R. State laws and actions
challenging certain health reforms. July
2014. Available at: http://www.ncsl.
org/research/health/state-laws-and-
actions-challenging-ppaca.aspx. Accessed
July 7, 2014.
6. US Census Bureau. Annual estimates
of the resident population for counties:
April 1, 2010 to July 1, 2013. May
2014. Available at: http://www.census.
gov/popest/data/counties/totals/2013/
CO-EST2013-01.html. Accessed June
20, 2014.
7. University of Wisconsin Population
Health Institute. County snapshot: Wy-
andotte, Kansas. 2014. Available at:
http://www.countyhealthrankings.org/
app/kansas/2014/rankings/wyandotte/
county/outcomes/overall/snapshot. Ac-
cessed June 20, 2014.
8. US Census Bureau. Annual estimates
of the resident population by sex, race,
and Hispanic origin: April 1, 2010 to
July 1, 2012. March 27, 2014. Available
at: http://www.census.gov/popest/data/
counties/asrh/2012/PEPSR6H.html.
Accessed June 20, 2014.
9. Fawcett S, Schultz J. Using the
Community Tool Box’s online docu-
mentation system to support participa-
tory evaluation of community health
initiatives. In: Minkler M, Wallerstein
N, eds. Community-Based Participatory
Research for Health: From Process to Out-
comes. San Francisco, CA: Jossey-Bass;
2008:219–224.
10. Fawcett S, Schultz J, Watson-
Thompson J, Fox M, Bremby R. Build-
ing multisectoral partnerships for popu-
lation health and health equity. Prev
Chronic Dis. 2010;7(6):A118.