Downloaded 136 times



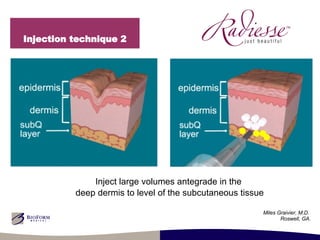
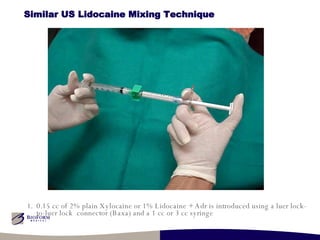
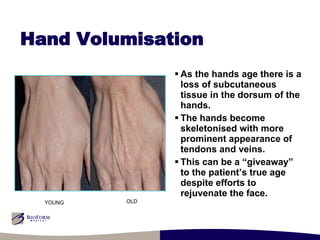

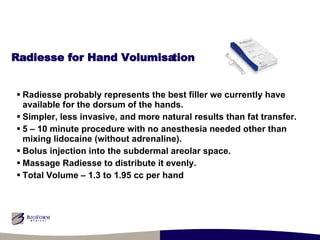
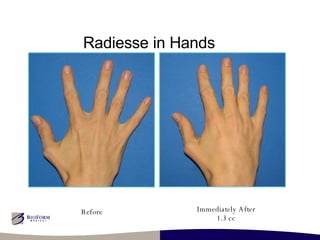
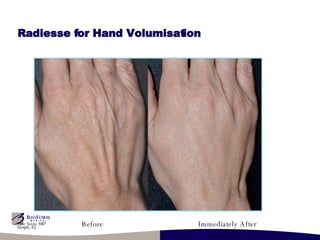

Dr. Patrick J. Treacy, a cosmetic doctor, presented advanced injection techniques including the use of Radiesse XL for facial and hand volumization at a meeting in London. The lecture emphasized the importance of patient comfort during procedures and introduced mixing lidocaine with Radiesse to reduce pain and prevent tissue distortion. Key benefits of Radiesse included its biocompatibility and effectiveness in treating age-related volume loss in hands.

















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





