More Related Content Similar to AD Pathology Paper Rajana 2014 Similar to AD Pathology Paper Rajana 2014 (20) 2. Structured Abstract:
Background: Alzheimer’s Disease (AD) affects millions of people worldwide, and
with our aging population, the prevalence of AD is only increasing. Recent research shows
that AD pathology begins in the brainstem even before clinical symptoms, such as memory
loss and impaired cognition, appear. The substantia nigra (SN) is a dopamine producing
nucleus in the brainstem closely tied to other nuclei that have shown changes in early AD,
such as the locus coeruleus. The present study analyzes changes in the SN by way of tau-
protein accumulation, a hallmark of AD, in brains of early AD patients using unbiased
stereology. Methods: Human brainstems from seven subjects aged 46-71 with early AD
were obtained from the Brain Bank of the Brazilian Aging Brain Study Group, fixed in
celloidin, and processed using immunohistochemistry for unbiased stereological analysis
to quantitatively characterize the tau-protein burden. Results: Although there was a small
sample size of only seven brains, there appears to be a positive relationship between tau
burden and age of patients, which is trending toward significance. There was no correlation
between Braak stage and tau burden. Conclusions and Further Research: The findings
are in line with recently published work describing an increase in tau burden with age,
independent of AD. However, the small sample size gives us little power when making
conclusions, and for this reason, an immediate expansion of sample size is necessary to
create a normative base for further studies of early AD in the SN.
3. I. Introduction
As of 2014, over 5 million individuals aged 65 and older in America have been
diagnosed with Alzheimer’s disease, along with an additional 200,000 individuals under 65
diagnosed with early-onset Alzheimer’s disease (Alz.org). Currently, one in nine people, or
11% of the population aged 65 or older has or will have Alzheimer’s disease (Alz.org). By
2030, senior citizens are expected to make up 19% of the American population, compared
to 12.4% in the year 2000, with the number of seniors doubling to 72.1 million individuals
(Administration on Aging). Because of the increasing number of individuals aged 65 and
older in the United States, the number of new cases for Alzheimer’s and other dementias is
predicted to double by the year 2050 (Alz.org).
As every individual ages, the brain changes, and they begin to develop plaques and
neurofibrillary tangles. The prevalence of plaques and neurofibrillary tangles in
Alzheimer’s disease, however, is purportedly much higher (Hardy 2002), and increases
with the progression of the disease. Plaques occur when pieces of the beta-amyloid protein,
which is a part of the membrane surrounding neurons, starts to come off the membrane
and clump together outside the cells. Since there is no genetic change in the amyloid beta
precursor protein, we know that plaques are caused by transcriptional or posttranslational
changes (Selkoe et. all 1988). Neurofibrillary tangles are caused by hyperphosphorylated
tau proteins inside cells. The tau gene codes for RNA, which in turn, codes for the tau
protein. The protein has several epitopes, which are activated and inactivated by
phosphorylation. This can be compared to the cockpit of a plane; each of the many buttons
controls a specific function, and can be turned on and off. The abnormally functioning tau
protein, which usually supports the microtubules (MTs) in neurons, no longer has the same
affinity for the MTs (Geschwind 2003). Subsequently, the MTs in neurons collapse,
combination of plaques and tangles impedes normal functions in cells, and eventually
precipitates cell death.
The hyperphosphorylated, and subsequently misfolded, tau protein spreads throughout
the brain following a characteristic pattern. The Braak staging system, initially published in
1991, is a qualitative method of categorizing the degree of AD pathology in postmortem
brains from stages I to VI (Braak and Braak 1991). For this study of changes in the brain in
early AD, brains with Braak stages 0 to II were used. In 1991, it was established that there
4. is little to no tau- positive neurofibrillary tangle burden in the neocortex, the upper part of
the cerebral cortex in early stages. Because the cerebral cortex houses areas dealing with
cognitive function, such as language, memory, motor commands, and spatial language, the
disease-defining symptoms of AD are not manifested until the later stages. The Braak
staging system is still used today, but was reviewed and modified in 2011 to include
changes in the locus coeruleus, a subcortical nucleus, in the early stages (Grinberg et. al
2011). This explains how disease pathology develops even before clinical symptoms
appear, and further research could lead to an effective treatment that targets AD before it
spreads into the neocortex.
The neuronal loss in AD originates in an area of the brainstem known as the
isodendritic core. The isodendritic core is made up of four main nuclei: the dorsal raphe,
locus coeruleus, parabrachial nucleus, , and the substantia nigra (SN). The substantia nigra
is affected in several neurodegenerative diseases, including in the early stages of
Parkinson’s disease (Braak 2003), and produces the neurotransmitter dopamine, which is
known to play a role in happiness and the brain’s reward system. Most dopamine-producer
neurons of the SN also harbor neuromelanin, a pigment that causes the characteristic dark
color of the SN.
As the disease progresses, the degree of dementia is closely related to neuronal loss in
AD patients. While we do know that neurofibrillary tangles and neuronal loss are hallmarks
of AD, we do not know if, or how, they are related. There is a gap of studies done of well-
characterized individuals to understand the two lesions in the context of one another. The
overall goal of the lab that this study was conducted at, the Grinberg Lab (Memory and
Aging Center, UCSF), is to quantitatively study this relationship between protein buildup
and neuronal loss throughout the four major nuclei of the isodendritic core using
innovative methods. My project, specifically, focuses on a nucleus of the isodendritic core
known as the substantia nigra, and this is further discussed below.
Despite all the efforts and money to put into understanding and curing AD over the last
three decades, including all kinds of sophisticated experimental models designed to mimic
the disease, excellent treatment results on drugs tried in these animal models and huge
efforts in human clinical trials using the same drugs, we are yet to find something to cure or
even delay the progression of AD. At this point, we must go back to the fundamentals of AD
5. pathology, and look at how the disease progresses in humans. Because there has been little
success in translating positive results from animal models to human models beyond early
stage clinical trials, it is important that we gain a thorough understanding of the way AD
functions in the human brain before identifying therapeutic targets and developing
treatments.
Currently, little data is available as a baseline of normative changes in the SN through
aging, so this study seeks to create a library of data for the pathology of AD in the SN.
Additionally, the changes in the SN during aging, such as the natural occurrence of tangles
and plaques, as well as neuronal loss, are still controversial. Since the SN is bilateral, it is
also not known if the build-up of tangles and plaques differs on the left and right sides
(Alho 2014)
In looking at the SN through the lens of AD, we employ a double staining technique to
identify both the tau-negative neurons, stained with gallocyanine, and the tau-positive
neurons, stained with CP13 to analyze changes in the SN with age and with progression of
AD (Theofilas 2014). We lack data on what characterizes the pathology of early AD in the
brainstem. The results contribute to a base of knowledge for imaging, clinical, and
anatomical studies of the SN in the early stages of AD. My hypothesis is that because the SN
is a part of the isodendritic core and connected to other nuclei of the isodentritic core
vulnerable to AD, there will also be changes in the SN in early AD. However, because of
what is known of Braak stages, where there is little protein burden in the early stages of
AD, there will be correlation between age and tau burden.
II. Methods:
Prior to my analysis of the tissue using unbiased stereology, the brainstem was cut into 60
micrometer sections and processed using immunohistochemistry and specific brain areas
were sampled according to BBBABSG protocol (Grinberg et al. 2007). A short summary of
this method follows.
6. a. Participants:
Age of time of death Case Braak Stage Gender
44 7020.12 0 Female
46 9379.13 2 Female
47 7678.13 0 Female
56 9526.12 1 Male
70 6664.12 1 Female
71 6366.13 0 Male
71 6931.12 2 Female
Brainstem tissue from 7 individuals obtained from the BBBABSG was used. Grinberg and
colleagues have described the BBBABSG protocol in detail.
b. Embedding and Sectioning
The brainstem was embedded in celloidin to reduce tissue distortion, by first
dehydrating it with progressively stronger ethanol solutions and then going through a
dessication process to strongly secure the tissue. When enough liquid has been removed
from the celloidin to reach an India rubber consistency, the blocks were sectioned using a
sliding microtome. Brainstems were sectioned alternately into one 300 micrometer and
five 60 micrometer sections. The thick sections are the odd-numbered sections, used to
calculate an unbiased estimate for the neuronal population of the six nuclei in the
isodendritic core. The even 60 micrometer sections, used to evaluate the tau protein
burden in each of the nuclei. A comparison of the burden in the early of late stages of AD, as
well as with controls, is done in the 60 micrometer sections. During the cutting process,
each section was photographed using an EOS 5D Mark II.
7. b. Staining and Immunohistochemistry
`The thin 60 micrometer sections were first stained using a monoclonal CP13
antibody, which stained for both cytoplasmic bound and extracellular phosphorylated tau.
Beyond this, they were counterstained overnight in 2.0 pH gallocyanine to stain the
nucleoli and create further contrast between tau positive neurons and surrounding cells.
Then, the sections were mounted to slides, coverslipped, and labeled by number.
c. Stereology in the Substantia Nigra
In terms of physical orientation, the SN is a bilateral nucleus located in the midbrain,
adjacent to the cerebral peduncles. It is divided into three parts: the par compacta, parts
diffusa, and pars reticulata. The pars compacta has the highest neuron density and is made
up of the largest, most pigmented neurons. The pars diffusa is not as dense, and has smaller,
less pigmented neurons, although there are some clusters of neurons resembling those
found in the pars compacta. Finally, the pars reticulata contains thick dendrites of the
neurons in the pars compacta region, as well as a few spread-out neurons lacking the
neuromelanin pigment.
Stereological analyses were performed using the StereoInvestigator program (MBF
StereoInvestigator v.10, MBF Bioscience, Williston, VT, USA). This set-up was comprised of
a motorized stage system, which allowed movement of the stage to view a different section
of the slide if necessary, a bright field microscope (Axio A2, Zeiss Microscopy, Thornwood,
NY, USA), and a color camera to facilitate use of the microscope on an external monitor.
9. the pilot study is to determine the minimum counting and sampling required to ensure
accuracy of sampling. In other words, the goal is to count enough cells with minimal work.
The resample-oversample process begins with an exhaustive analysis of each and every
site in the tissue in predetermined blocks. After this, the program uses a formula to
determine the parameters such that the counter is getting the most accurate results with
the least amount of work possible.
In the oversample parameters, the grid size was automatically generated, and the
optical fractionator top guard zone was set as 5 micrometers and dissector height at 25
micrometers, based on the minimum section thickness. Section thickness was measured
manually using a motor to go through the z-axis each time a neuron was counted, and the
measure used in calculations was an average of all thickness measurements. New resample
parameters were established upon running the probe and evaluating the data plotted in the
resample oversample graph.
Figure 2: This graph, generated using the Resample Oversample probe in
StereoInvestigator, was generated in Microsoft Excel. It shows how close the
neuronal estimates are in counting every interval of dissector sites, from every
site to every 20th site. According to this graph, the optimal interval is every 3rd
dissector site, because the estimates using one, two, and three counters are
closest to each other. Therefore, counting every third dissector site will allow us
to maintain accuracy with minimal work.
10. The pilot study is recounted according to the parameters given by the resample
oversample graph, and the data is compared to determine how close the resample and
oversample estimates of neuronal populations are. Theoretically, they should be the same,
because the parameters are calculated such that the same level of accuracy is maintained,
even with fewer dissector sites. If the estimates are significantly different, the oversample-
resample process is repeated until the estimates are reliable and can be used to count
additional cases using the same parameters.
A CP13-negative neuron is stained light brown because of the neuromelanin the SN,
while the nucleus and nucleolus are stained blue because of the gallocyanine stain. Only
neurons where the nucleus and nucleolus are clearly visible are counted, because the
sectioning process can cut off neurons along the z-axis, creating fragments that can skew
neuronal estimates if counted as neurons. Additionally, using the nucleolus and nucleus as
markers in stereology is in line with the staining techniques described in the staining
section. In comparison to the CP13-negative neurons, CP13-postive neurons are covered in
a dark brown blanket of CP13 stain. The staining is approximately uniform across the cell
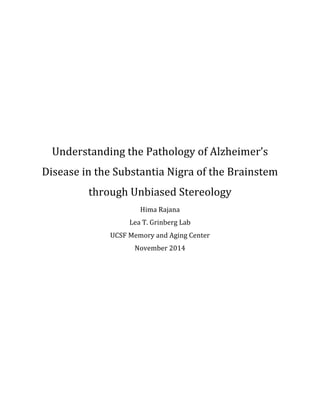
Figure 2: The substantia nigra is traced at 5x. This image is the complete right
side of the nucleus. The characteristic wavy structure, where the contour goes
in and out, following the lines of the SN, is visible here.
12. In order to ensure that each neuron is counted a maximum of one time when the
program places the dissector randomly, any neurons in contact with the red-edged part of
the square (see below figure for reference) were not counted, even if they meet the criteria
according to the previous paragraph. Any neurons touching the green-edged part of the
square, whether completely or partially inside the square, are counted. Additionally,
several dissectors intersected with the border of the contour, as shown in the image below.
Figure 5: The substantia nigra contour is broken into many counting frames, and the
dissector site, where the user counts neurons, is consistently in the bottom left
corner. The smaller the counting frame, the more dissector sites to count.
Figure 5: The gallocyanine-stained neurons are smaller, and a darker area of
the nucleus and nucleolus, where the stain is deeper, is visible.
13. A
At 40x, it is quite difficult to tell where the dissector is in relation to the contour as a whole
and relative to the position of the slide, so having an overall map of the contours indicating
where the dissector is tells us how the dissector falls on the contour, and consequently
which neurons can be counted and which ones fall outside the previously delineated
contour is necessary. The Macroview feature on Stereology investigator helps overcome
this issue, as shown in the image below.
e. Statistical Analysis
The resample oversample probe used a formula embedded in the program to calculate
the appropriate interval for the resample. The coefficients of error for the tau-positive
neuronal estimates were calculated using the prediction methods from the
StereoInvestigator, the Gundersen and Schmitz-Hof’s coefficient of error measurements.
Figure 6: The Macroview feature, located in the upper left hand corner, shows
the entire contour, with a smaller box indicating where the dissector site,
displayed on the right side at 40x, is in relation to the whole contour. Because of
this, we know to count only the neurons on the left side of the orange contour
line, since they are the only ones inside the contour.
14. These measurements are useful for determining the precision of neuronal estimates, and
have been described previously (Gundersen et al. 1999; Schmitz, 1998). Planned statistical
analysis for further studies follows in the further research section.
III. Results
The 60 micometer gallocyanine-stained sections fulfilled the basic requirements of
unbiased design-based stereology, which has proven to be the optimal method for cell
counting time and again for its abilities to detect the most minute cell group differences
(Schmitz and Hof 2005). Every cell inside the region of interest had equal opportunity to be
selected for counting for two main reasons. First, the serial sectioning of the brainstem
allowed us to evaluate the full thickness of the SN along the z-axis, so we did not miss any
neurons. Second, the boundaries of the SN were easily detectable, and we were able to
draw contours around all of them. Although the sections were supposedly all 60
micrometers thick, thickness was measured to account for any shrinkage or discrepancies
in cutting. The section thickness of each case was an average of the measured section
thicknesses or each dissector sites. This helped account for any folding, waviness, or
Table 1: This table shows all of the dta
15. warping of the tissue. The mean section thickness across all cases was 48.7 micrometers
with a standard deviation of 0.28 micrometers.
Through the resample oversample probe, I determined that I could count every third
dissector site without losing accuracy. Due to the experimental nature of stereology, I had
to conduct the oversample-resample four times before receiving satisfactory results. I was
then able to use these parameters to count six other cases. Originally, I counted not CP13-
negative cells, in addition to the data of CP13 positive neurons presented in this paper.
Unfortunately, there were problems with the counterstain in the immunohistochemistry
process, so these results have been deemed unreliable. Both the resample-oversample and
the CP13-negative cell issues will be explained further in the discussion section.
Of the seven cases counted, four appeared to have no tau burden, and the remaining
three had similar burdens. After blind counting, the Braak stages and age of patient were
matched with the data, and we tested for correlation. Based on this data, there is no
correlation between tau burden and Braak stage, as all of the cases that had tau burdens
were Braak stage 0 or 1. While the sample size is too small to claim a correlation between
tau burden and age, there is a positive trend between age and tau burden. Out of three
patients older than 65 at time of death, each had a different Braak stage of 0, 1, and 2, but
two of the three showed similar presence of neurofibrillary tangles. Out of the 4 patients
under age 65 at time of death, only 1 patient showed any tau burden, and the level was
similar to the two patients over 65. Thus, the positive correlation between age and tau
burden is trending towards significance, and the immediate course of action would be to
expand the sample size of this study. This would allow us to determine if the correlation is
simply the result of a small sample size or can be supported with further data.
IV. Discussion
As our worldwide population ages, the prevalence of neurodegenerative diseases,
especially dementia and Alzheimer’s, is increasing. At the same time, the scientific
community’s efforts to work towards a cure, or even treatment of Alzheimer’s disease, have
been stalled by the difficult transition from animal models to human models. Something
about human brains is different enough that whatever semblance of progress is achieved in
16. animal models does not translate to human models. For this reason, it is necessary to study
the way AD progresses in humans specifically, because there is a gap of knowledge that can
only be filled by using postmortem brain tissue help characterize early stages of AD.
Currently, these is a lack of unbiased data on the substantia nigra, a key nuceus of the
isodendritic core, known chiefly for the dark pigment as a result of dopamine production.
Although we know of some changes in the other nuclei of the isodendritic core, including
the locus coeruleus, little is known about the SN in the context of AD. Because one of the
hallmarks of AD is tau protein buildup, we analyzed protein buildup in the SN using
unbiased stereology in a post-mortem sample of 7 adults aged 46-71 at time of death.
Quantitative neuropathological methods are time consuming, tedious and usually biased
due to the enourmous amont of neurons in the brain. Design-based stereology is
transforming the way quantitative neuropathology is performed, allowing us to make
predictions for the neuron number and density of a tissue without counting each and every
neuron through an establishment of parameters using a resample-oversample process. In
addition, the randomness of stereology allows us to make unbiased measurements and be
able to trust in the validity of results.
Although there seemed to be no discernable relationship between tau burden and
Braak stage, there does appear to be a positive relationship between age and tau burden,
trending toward significance. This is in line with a very recently published paper on tau
buildup as related to age in the brainstem. Crary and colleagues suggest the use of a new
term: primary age-related tauopathy (PART) to describe tau build up in the brain that
seems to be tied only to age (Crary et. al. 2014). Pathologically, this can be distinguished
from AD, frontotemporal dementia, or other neurodegenerative diseases by the lack of the
beta-amyloid plaques. Although the lack of beta-amyloid plaques points o a diagnoses is
early AD, there are some clinical differences, since PART usually has a lesser cognitive
impact. Looking at PART through the lens of AD, Crary and colleagues found that many
patients with mild-to-moderate neurofibrillary burden similar to early stage AD lacked the
beta amyloid plaques characteristic of AD. Thus, the neurofibrillary tangles may be
involved in a non AD aging related process. The incidence of PART was much higher in
older patients, which supports the possible positive relationship between tau burden and
age.
17. Even though my findings are supported by Crary’s work, it is difficult to confirm
anything working with such a small sample size, especially in humans. Humans are such
diverse, varied, and unique beings that variation becomes not the exception but the norm.
For this reason, many cases are necessary to draw a general conclusion that can be applied
to the entire population, and this study does not have the high sample size. Because of the
gap of knowledge considering the substantia nigra and AD, we are unable to calculate the
exact number of cases needed to have power in terms of statistics. The biggest reason for
the small sample size in this study is the difficulty of procuring human brains with the early
AD diagnosis. This kind of analysis can only be done post mortem, and processing the
brains for stereology in human models takes a very long time compared to rat brains,
which are much smaller. It is still important to study this in humans because the disease
manifests itself in humans. Therefore, the main goal of this study is not necessarily to make
sweeping conclusion about the nature of AD in the SN, but rather to build a knowledge base
to characterize the SN in early AD. As I write this paper, I am in the process of increasing
sample size, and by the end of this winter, I should have around 20 cases, which gives much
more power in terms of being representative of early AD brains, than seven.
Stereology is an experimental process in and of itself, because the Resample
Oversample probe allows the user to tailor the program to the type of tissue being counted.
Prior to any stereological analysis of multiple cases, it is necessary to run a complex pilot
study to ensure that results are not only reliable, but can also be replicated in other labs. As
mentioned in the results sections, I had to conduct the oversample probe four times to get
satisfactory results. The algorithm in StereoInvestigator recommended that I count every
third dissector site three times in all four occurrences. Theoretically, the overall neuronal
estimates for the oversample and the resample should be the same, but that wasn’t the case
in the initial oversample. Throughout the process, issues with inconsistent neuron
estimates, inconsistent thickness measurements, and inaccurately drawn contours
prompted me to conduct the analysis again. Finally, on the fourth round, I had reliable
parameters, which I then used to count six additional cases.
I originally counted both CP13 positive and CP13 negative neurons. Upon review of the
results and comparisons to other stereological estimates of substantia nigra neuron
population, my numbers were only 10-20% of others’ results. We evaluated my criteria for
18. counting neurons and the counting parameters and eventually concluded that the
inaccurate results were a result of a faulty counterstain. After the CP13 stain was applied to
the sections, they were counterstained in a gallocyanine wash to illuminate the CP13
negative neurons. The 60 micrometer sections may have been slightly too thin for the
harsh chemicals, or may have reacted negatively to the tested concentration of detergent in
the solution. In order to account for this in further studies, neuronal estimates will now be
measuring from only the thick 300 micrometer sections of each case. As of now, the
staining and stereology protocol has been optimized for the 300 micrometer sections, with
consistently reliable results. As we have learned from this study, the CP13 stain done
through immunohistochemistry works well on the thin 60 micrometer sections. As per the
cutting protocol followed by the Grinberg lab, 300 micrometer sections and 60 micrometer
sections are cut alternately, so the 300 micrometer sections are an accurate representation
of the 60 micrometer sections. In order to understand the relationship and dynamic
between neuronal loss and tau protein accumulation, we will now utilize a combination of
data from the 300 micrometer sections, for neuronal estimates, and 60 micrometer
sections, for protein burden estimates.
V. Conclusions and Further Research
This study was an investigation of the human substantia nigra in the early stages of
AD. There is a positive trend between age and tau protein accumulation, and as of now, no
relationship between Braak stage and tau burden. However, the small sample size gives us
very little power in making applicable conclusions. The immediate next step is to increase
the sample size in order to run appropriate statistical analysis. The analysis will test the
individual correlations by comparing anatomical changes, such as inclusion burden, with
age and Braak stage using linear regression analysis. The regression models will include
indicators for AD group as well as age at death.
Additionally, in order to investigate the role of the substantia nigra in AD, and
perhaps look further into the still undiscovered relationship between SN protein burden
and Braak stage, we can use neuronal estimates from the 300 micrometer sections.
Comparing the overall neuronal estimates to the tau-positive neuron estimates would
20. Bibliography
"Administration on Aging (AoA)." Aging Statistics. Administration for Community Living, 31
Dec. 2000. Web. 09 Nov. 2014.
Alho, Ana Tereza Di Lorenzo. "Three-dimensional and Stereological Characterization of the
Human Substantia Nigra during Aging." (2014): n. pag. Web. 2 Nov. 2014.
Association, Alzheimer's. "2014 Alzheimer’s Disease Facts and Figures." Alzheimer’s &
Dementia 10.2 (2014): n. pag. Alz.org. Alzheimer's Association. Web. 21 Sept.
2014.
Braak, H., and E. Braak. "Neuropathological Stageing of Alzheimer-related Changes." Acta
Neuropathologica 82.4 (1991): 239-59. Web. 21 Oct. 2014.
Braak, Heiko, K. Del Tredi, U. Rub, and RA De Vos. "Staging of Brain Pathology Related to
Sporadic Parkinson's Disease." The Neurobiology of Aging 24.2 (2003): 197-211.
Web. 7 Oct. 2014.
Büttner-Ennever, Jean A., A. K. E. Horn, and Jerzy Olszewski. Olszewski and Baxter's
Cytoarchitecture of the Human Brainstem. N.p.: Karger, n.d. Print.
Crary, John F., John Q. Trojanowski, Julie A. Scheider, and Jose F. Abisambra. "Primary Age-
related Tauopathy (PART): A Common Pathology Associated with Human Aging."
Acta Neuropathologica (2014): n. pag. Web. 1 Nov. 2014.
Geschwind, Daniel H. "Tau Phosphorylation, Tangles, and Neurodegeneration: The Chicken
or the Egg?" Neuron 40 (2003): 457-60. Web. 15 Sept. 2014.
Grinberg, Lea Tenenholz, Renata Eloah Lucena Ferretti, José Marcelo Farfel, Renata Leite,
Carlos Augusto Pasqualucci, Sérgio Rosemberg, Ricardo Nitrini, Paulo Hilário
Nascimento Saldiva, and Wilson Jacob Filho. "Brain Bank of the Brazilian Aging
Brain Study Group—a Milestone Reached and More than 1,600 Collected Brains."
Cell and Tissue Banking 8.2 (2007): 151-62. Web. 18 Sept. 2014.
Grinberg, Lea Tenenholz, Udo Rueb, and Helmut Heinsen. "Brainstem: Neglected Locus in
Neurodegenerative Diseases." Frontiers in Neurology 2 (2011): n. pag. Web. 3 Oct.
2014.
Gundersen, H. J. G., E. B. V. Jensen, K. Kieu, and J. Nielsen. "The Efficiency of Systematic
Sampling in Stereology - Reconsidered." Journal of Microscopy 193.3 (1999): 199-
211. Web. 1 Nov. 2014.
21. Hardy, J. "The Amyloid Hypothesis of Alzheimer's Disease: Progress and Problems on the
Road to Therapeutics." Science 297.5580 (2002): 353-56. Web. 10 Sept. 2014.
Kazee, Ann Marie, Christopher Cox, and Eric K. Richfield. "Substantia Nigra Lesions in
Alzheimer Disease and Normal Aging." Alzheimer Disease & Associated Disorders
9.2 (1995): 61-67. Web. 19 Oct. 2014.
"Medical Neurosciences." Medical Neurosciences. University of Wisconsin Madison, n.d.
Web. 13 Oct. 2014.
Schmitz, C., and P.r. Hof. "Design-based Stereology in Neuroscience." Neuroscience 130.4
(2005): 813-31. Web. 29 Oct. 2014.
Schmitz, Christoph. "Variation of Fractionator Estimates and Its Prediction." Anatomy and
Embryology 198.5 (1998): 371-97. Web. 1 Nov. 2014.
Selkoe, Dennis J. "F3-Amyloid Precursor Protein of Alzheimer Disease Occurs as 110- to
135-kilodalton Membrane-associated Proteins in Neural and Nonneural Tissues."
Medical Sciences 85 (1988): 7341-345. Web. 14 Oct. 2014.
Theofilas, Panos, Livia Polichiso, Xuehua Wang, Luzia C. Lima, Ana T.l. Alho, Renata E.p.
Leite, Claudia K. Suemoto, Carlos A. Pasqualucci, Wilson Jacob-Filho, Helmut
Heinsen, and Lea T. Grinberg. "A Novel Approach for Integrative Studies on
Neurodegenerative Diseases in Human Brains." Journal of Neuroscience Methods
226 (2014): 171-83. Web. 27 Sept. 2014.
Yoshiyama, Yasumasa, Bin Zhang, and Jennifer Bruce. "Reduction of Detyrosinated
Microtubules and Golgi Fragmentation Are Linked to Tau-induced Degeneration
in Astrocytes." Journal of Neuroscience 23.33 (2003): 10662-0671. Web. 16 Aug.
2014.