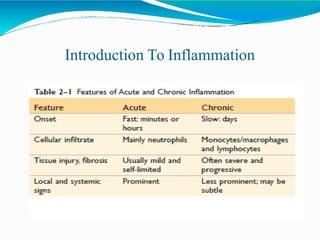
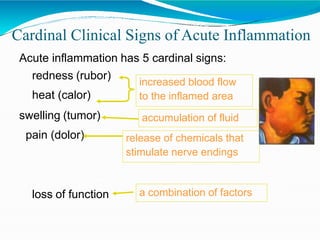
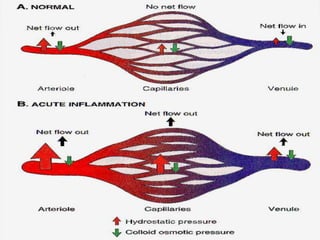
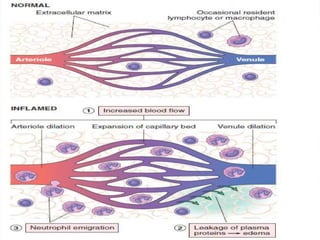
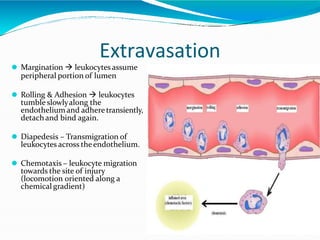
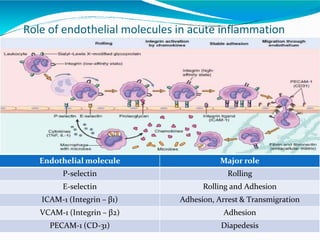
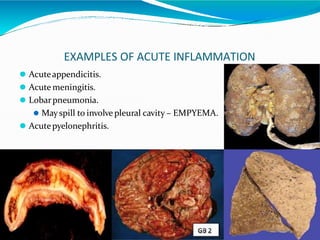
Acute inflammation is characterized by five signs: redness, heat, swelling, pain, and loss of function. It involves both vascular and cellular events over a short period of time. The vascular events include increased blood flow and permeability, which leads to fluid leakage. The cellular events involve leukocyte recruitment to the site through adhesion molecules and chemotaxis, followed by activation and phagocytosis of microbes. Acute inflammation can manifest morphologically as serous, fibrinous, purulent or hemorrhagic inflammation. It typically resolves through resolution or repair, but can also lead to suppuration or progress to chronic inflammation.





































![salivary gland journal.finalppt [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/salivaryglandjournal-250321010241-e4b72dc6-thumbnail.jpg?width=640&height=640&fit=bounds)


























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






