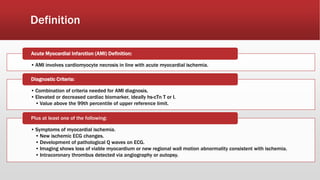
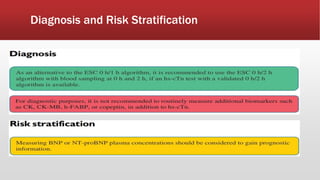
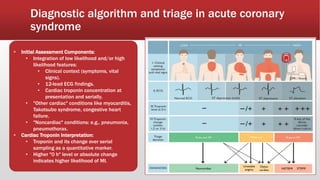
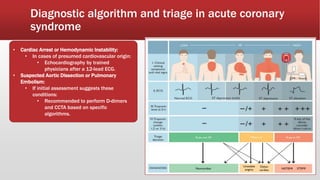
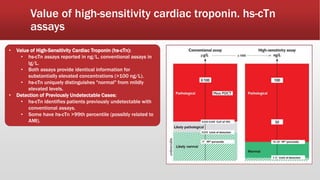
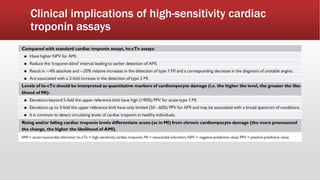
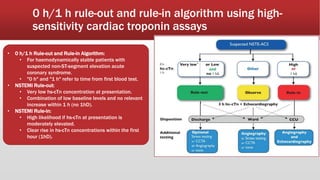
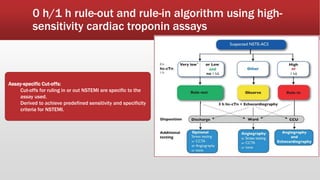
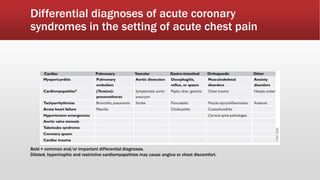
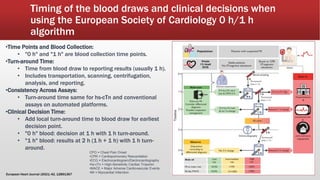
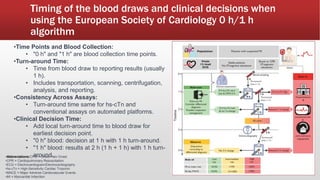
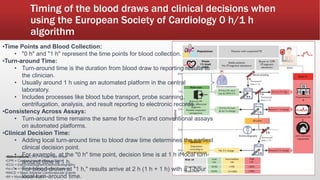
Acute MI management involves defining AMI, outlining diagnostic criteria, discussing diagnostic algorithms and triage, reviewing the value of high-sensitivity cardiac troponin assays, and exploring the clinical implications of using such assays. Key points include: AMI involves cardiomyocyte necrosis due to acute ischemia, diagnostic criteria include cardiac biomarker elevation and symptoms, and high-sensitivity troponin assays can identify previously undetectable cases and provide quantitative data on likelihood of MI. The 0h/1h rule-out and rule-in algorithm uses assay-specific cut-offs for troponin to determine likelihood of NSTEMI.















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














