Download free for 30 days
Sign in
Upload
Language (EN)
Support
Business
Mobile
Social Media
Marketing
Technology
Art & Photos
Career
Design
Education
Presentations & Public Speaking
Government & Nonprofit
Healthcare
Internet
Law
Leadership & Management
Automotive
Engineering
Software
Recruiting & HR
Retail
Sales
Services
Science
Small Business & Entrepreneurship
Food
Environment
Economy & Finance
Data & Analytics
Investor Relations
Sports
Spiritual
News & Politics
Travel
Self Improvement
Real Estate
Entertainment & Humor
Health & Medicine
Devices & Hardware
Lifestyle
Change Language
Language
English
Español
Português
Français
Deutsche
Cancel
Save
Submit search
EN
Uploaded by
Thorsang Chayovan
115 views
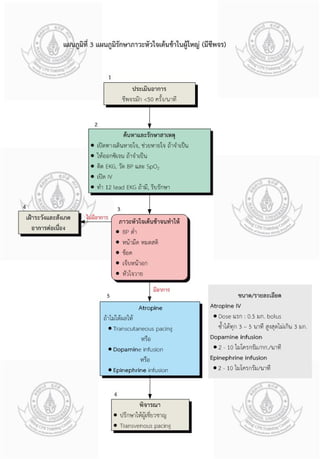
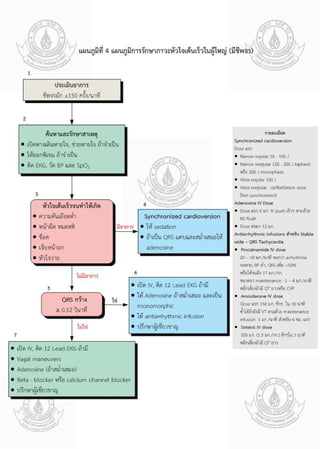
ACLS Thai
ACLS
Health & Medicine
◦
Read more
0
Save
Share
Embed
Embed presentation
Download
Download to read offline
1
/ 4
2
/ 4
3
/ 4
4
/ 4
More Related Content
PDF
COVID-19 Findings on Chest CT
by
Thorsang Chayovan
PPTX
Dyspepsia endoscopy guideline
by
Thorsang Chayovan
PPTX
Common respiratory problems
by
Thorsang Chayovan
PPT
Avascular necrosis
by
Thorsang Chayovan
PPT
Shoulder injury
by
Thorsang Chayovan
PPTX
Pediatric pneumonia Thai
by
Thorsang Chayovan
PDF
Pediatric upper urinary tract infection in Thai
by
Thorsang Chayovan
PDF
Tokyo guidelines for cholangitis and cholecystitis
by
Thorsang Chayovan
COVID-19 Findings on Chest CT
by
Thorsang Chayovan
Dyspepsia endoscopy guideline
by
Thorsang Chayovan
Common respiratory problems
by
Thorsang Chayovan
Avascular necrosis
by
Thorsang Chayovan
Shoulder injury
by
Thorsang Chayovan
Pediatric pneumonia Thai
by
Thorsang Chayovan
Pediatric upper urinary tract infection in Thai
by
Thorsang Chayovan
Tokyo guidelines for cholangitis and cholecystitis
by
Thorsang Chayovan
More from Thorsang Chayovan
PDF
The role of ercp in diseases of the biliary tract and pancreas
by
Thorsang Chayovan
PDF
Role of endoscopy in dyspepsia
by
Thorsang Chayovan
PDF
Role of endoscopy in choledocholithiasis
by
Thorsang Chayovan
PDF
Pneumonia in children
by
Thorsang Chayovan
PDF
คู่มือเวชปฏิบัติหัตถการ
by
Thorsang Chayovan
PDF
Febrile neutropenia in children
by
Thorsang Chayovan
PDF
Exanthematous fever in children
by
Thorsang Chayovan
PDF
Diseases of the rectum and anal canal in Thai
by
Thorsang Chayovan
PDF
Thai PALS manual 2009
by
Thorsang Chayovan
PDF
NEJM Cholecystitis
by
Thorsang Chayovan
PDF
Thai hemorrhagic stroke guideline 2008
by
Thorsang Chayovan
PDF
A child with fever and seizure in Thai
by
Thorsang Chayovan
PDF
Children with recurrent chest infection
by
Thorsang Chayovan
PDF
Brain and behavior in Thai
by
Thorsang Chayovan
PDF
Approach to the child with recurrent infections
by
Thorsang Chayovan
PDF
Acute cholecystitis and acute cholangitis
by
Thorsang Chayovan
PDF
Acute cholangitis note
by
Thorsang Chayovan
PDF
CPG Thai Tuberculosis 2543
by
Thorsang Chayovan
PDF
CPG Thai Stroke infarct retrieved since 2555
by
Thorsang Chayovan
PDF
Thai update on pulmonary hypertension 2009
by
Thorsang Chayovan
The role of ercp in diseases of the biliary tract and pancreas
by
Thorsang Chayovan
Role of endoscopy in dyspepsia
by
Thorsang Chayovan
Role of endoscopy in choledocholithiasis
by
Thorsang Chayovan
Pneumonia in children
by
Thorsang Chayovan
คู่มือเวชปฏิบัติหัตถการ
by
Thorsang Chayovan
Febrile neutropenia in children
by
Thorsang Chayovan
Exanthematous fever in children
by
Thorsang Chayovan
Diseases of the rectum and anal canal in Thai
by
Thorsang Chayovan
Thai PALS manual 2009
by
Thorsang Chayovan
NEJM Cholecystitis
by
Thorsang Chayovan
Thai hemorrhagic stroke guideline 2008
by
Thorsang Chayovan
A child with fever and seizure in Thai
by
Thorsang Chayovan
Children with recurrent chest infection
by
Thorsang Chayovan
Brain and behavior in Thai
by
Thorsang Chayovan
Approach to the child with recurrent infections
by
Thorsang Chayovan
Acute cholecystitis and acute cholangitis
by
Thorsang Chayovan
Acute cholangitis note
by
Thorsang Chayovan
CPG Thai Tuberculosis 2543
by
Thorsang Chayovan
CPG Thai Stroke infarct retrieved since 2555
by
Thorsang Chayovan
Thai update on pulmonary hypertension 2009
by
Thorsang Chayovan
Recently uploaded
PDF
Regal Best Kidney Multispecialty Hospital
by
sekhardigitalmarketi
PPT
RSV Prophylaxis Unveiled: What Healthcare Providers Need to Know
by
PVI, PeerView Institute for Medical Education
PDF
स्वास्थ्यकर्मी_पारिश्रमिक_तथा_सेवा_सुविधा_प्रतिवेदन_२०८२
by
Public Health Concern Nepal
PDF
The Special Senses Organs in human body
by
alfrjanymalk66
PPT
Forging New Paths With Earlier Use of ADCs in Breast Cancer: From Clinical Br...
by
PVI, PeerView Institute for Medical Education
PPTX
Pressure ulcer Internal KPIs results for July,2024.pptx
by
profyasser95
PPTX
Imaging of benign focal lesions of the Liver
by
Dr. Aryan (Anish Dhakal)
PPTX
LECT 7A DISEASES CAUSED BY CHEMICAL AND ENVIRONMENTAL FACTORS.pptx
by
AlphonceIzengo
PPT
Many Roads to Myeloma Remission: Making Sequential Choices With BCMA and Non-...
by
PVI, PeerView Institute for Medical Education
PPTX
Communication and utilization of research.pptx
by
Preeti Kulshreshtha
PPTX
case control study for Community Medicine.pptx
by
Dr.Bharti Koria
PPTX
SPS_PE_LAB 2_Liquid Operation-Centrifugation.pptx
by
supriyabhagwatsps
PPTX
Transport of Oxygen& CO2.pptx by dr ambareesha
by
Dr K Ambareesha Goud PhD
PPT
New Kids on the Block in mHSPC: Personalising Approaches Through Emerging Pre...
by
PVI, PeerView Institute for Medical Education
PDF
RETINAL VEIN OCCLUSION; CRVO & BRVO types, pathophysiology, diagnosis & manag...
by
SamikshaRai22
PPTX
Types of Communication Disorders SLP lecture 3.pptx
by
Dr Zonera Khalid PT
PPTX
Chronic Viral Hepatitis HEP B HEP C HEP D
by
NAWEEN KUMAR
PDF
The Challenges of Choice in First-Line EGFRm NSCLC: Practical Guidance on Opt...
by
PVI, PeerView Institute for Medical Education
PPTX
Unit- II (Bioavaliability & Bioequivalence).pptx
by
UditiHanda
PPTX
Updated PALS slides 2025 guidelines.pptx
by
drabrehman121
Regal Best Kidney Multispecialty Hospital
by
sekhardigitalmarketi
RSV Prophylaxis Unveiled: What Healthcare Providers Need to Know
by
PVI, PeerView Institute for Medical Education
स्वास्थ्यकर्मी_पारिश्रमिक_तथा_सेवा_सुविधा_प्रतिवेदन_२०८२
by
Public Health Concern Nepal
The Special Senses Organs in human body
by
alfrjanymalk66
Forging New Paths With Earlier Use of ADCs in Breast Cancer: From Clinical Br...
by
PVI, PeerView Institute for Medical Education
Pressure ulcer Internal KPIs results for July,2024.pptx
by
profyasser95
Imaging of benign focal lesions of the Liver
by
Dr. Aryan (Anish Dhakal)
LECT 7A DISEASES CAUSED BY CHEMICAL AND ENVIRONMENTAL FACTORS.pptx
by
AlphonceIzengo
Many Roads to Myeloma Remission: Making Sequential Choices With BCMA and Non-...
by
PVI, PeerView Institute for Medical Education
Communication and utilization of research.pptx
by
Preeti Kulshreshtha
case control study for Community Medicine.pptx
by
Dr.Bharti Koria
SPS_PE_LAB 2_Liquid Operation-Centrifugation.pptx
by
supriyabhagwatsps
Transport of Oxygen& CO2.pptx by dr ambareesha
by
Dr K Ambareesha Goud PhD
New Kids on the Block in mHSPC: Personalising Approaches Through Emerging Pre...
by
PVI, PeerView Institute for Medical Education
RETINAL VEIN OCCLUSION; CRVO & BRVO types, pathophysiology, diagnosis & manag...
by
SamikshaRai22
Types of Communication Disorders SLP lecture 3.pptx
by
Dr Zonera Khalid PT
Chronic Viral Hepatitis HEP B HEP C HEP D
by
NAWEEN KUMAR
The Challenges of Choice in First-Line EGFRm NSCLC: Practical Guidance on Opt...
by
PVI, PeerView Institute for Medical Education
Unit- II (Bioavaliability & Bioequivalence).pptx
by
UditiHanda
Updated PALS slides 2025 guidelines.pptx
by
drabrehman121
Download