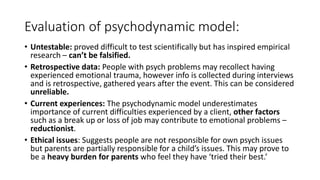
The document discusses various theories of abnormality, including deviation from social norms, failure to function adequately, and biological, psychodynamic, and behavioral approaches. It highlights the role of context and culture in defining abnormal behavior, the impact of mental disorders on daily life, and various intervention strategies. Additionally, it critiques these models for their limitations, such as reductionism and ethical concerns related to treatment methods.

























![Gardner academy jul_2012,_drug_use_and_abuse-1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/gardneracademyjul2012druguseandabuse-11-121002100444-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)