INTRODUCTION
Definition: bleedingfrom the uterine body that is abnormal in
frequency, duration and amount arising in the absence of
pregnancy.
Worlwide prevalence : 3-30%
The reasons for the wide spectrum of estimates are unclear but vary with
age, being higher in adolescents and in the fifth decade of life, and
varying somewhat with country of origin.
Approximately one third of women are affected at some time in their life.
In India, the prevalence of AUB is around 17.9%
FIGO., 2018
FOGSI, GCPR., 2016
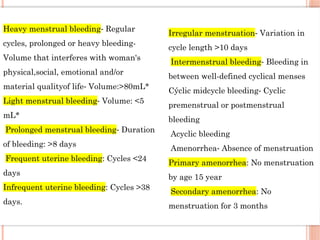
Heavy menstrual bleedingRegular
⁃
cycles, prolonged or heavy bleeding-
Volume that interferes with woman's
physical,social, emotional and/or
material qualityof life Volume:>80mL*
⁃
Light menstrual bleeding Volume: <5
⁃
mL*
Prolonged menstrual bleeding Duration
⁃
of bleeding: >8 days
Frequent uterine bleeding: Cycles <24
days
Infrequent uterine bleeding: Cycles >38
days.
Irregular menstruation Variation in
⁃
cycle length >10 days
Intermenstrual bleeding Bleeding in
⁃
between well-defined cyclical menses
Cýclic midcycle bleeding Cyclic
⁃
premenstrual or postmenstrual
bleeding
Acyclic bleeding
Amenorrhea Absence of menstruation
⁃
Primary amenorrhea: No menstruation
by age 15 year
Secondary amenorrhea: No
menstruation for 3 months
5.
Intermenstrual bleeding(IMB) occurs between clearly defined cyclical
and predictable menses.
Such bleeding may occur at random times or may manifest in a
predictable fashion at the same day in each cycle.
Heavy menstrual bleeding (HMB) , a symptom (not a diagnosis)
defined as excessive menstrual blood loss, which interferes with a
women’s physical, social, emotional and/or material quality of life.
(Definition proposed by UK National institute for health and care excellence and adopted by FIGO)
FIGO guidelines ., 2018
6.
Pathophysiology
Physiological mechanismof hemostasis in normal menstruation are:
• Platelet adhesion formation
• Formation of platelet plug with fibrin to seal the bleeding vessels
• Localized vasoconstriction
• Regeneration of endometrium
• Biochemical mechanisms involved are:
– Increased endometrial ratio of PGF2 a / PGE2. PGF2a causes vasoconstriction
– Progesterone increases the level of PGF2 a from arachidonic acid
– Endothelin (a powerful vasoconstrictor) is also increased.
– In anovulatory cycles there is decreased synthesis of PGF2 a and the ratio of PGF2 a /
PGE2 is low.
PG-F2alpha & thromboxane – vasoconstrictors
PGE2 & PGI2 - vasodilators
7.
Infancy Prepubertal AdolescentReproductive Perimenopausal Postmenopausal
Maternal
estrogen
withdrawal
Vulvovaginitis Anovulation Exogenous Anovulation Atrophy
Vaginal foreign
body
Exogenous
hormone
use
Pregnancy Fibroids Endometrial polyp
Precocious
puberty
Pregnancy Anovulation Polyps Endometrial
cancer
Tumor Coagulopat
hy
Fibroids Thyroid
dysfunction
Hormonal therapy
Polyps Other tumors:
vulvar, vaginal,
cervical
Thyroid
dysfunction
CAUSES OF AUB BY AGE GROUP
Berek $ Novak’s 16th
edition
8.
ACUTE VERSUS CHRONICNON-GESTATIONALAUB IN THE
REPRODUCTIVE YEARS
• CHRONIC AUB is defined as bleeding from the uterine corpus that is
abnormal in duration, volume, frequency and/ or regularity and has been
present for preceding 6 months.
• ACUTE AUB is defined as an episode of heavy bleeding that, in the opinion
of the clinician, is of sufficient quantity to require immediate intervention to
minimize or prevent further blood loss.
• Acute heavy menstrual bleeding may present in the context of existing chronic
AUB or can occur in the absence of such a background history.
FIGO guidelines ., 2018
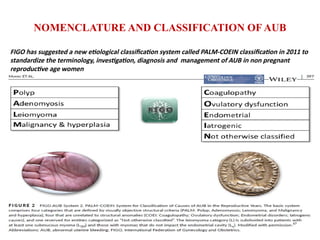
NOMENCLATURE AND CLASSIFICATIONOF AUB
FIGO has suggested a new etiological classification system called PALM-COEIN classification in 2011 to
standardize the terminology, investigation, diagnosis and management of AUB in non pregnant
reproductive age women
11.
AUB-P ; POLYPS(8-35 %)
• Endometrial polyp are soft, fleshy intrauterine growths, composed of
endometrial glands, fibrous stroma, and surface epithelium
• Most commonly found in reproductive-age Women
• Present with HMB, AUB, IMB or postcoital bleeding.
• The exact cause of polyps is unknown, but possible etiologies include genetic,
biochemical, and hormonal factors
• Estrogen and progesterone have been implicated in their growth, and higher
receptor levels are noted within polyps compared with adjacent normal
endometrium
• These hormones elongate endometrial glands, stromal tissue, and spiral arteries,
leading to the characteristic polypoid appearance.
12.
Diagnosis
• The maindiagnostic tools for endometrial polyp evaluation
TVS with color Doppler, SIS, and hysteroscopy.
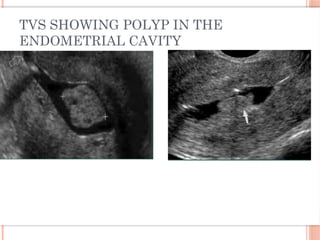
• TVS - endometrial polyp may appear as a nonspecific endometrial thickening
or as a round or elongated hyperechoic focal mass within the endometrial cavity.
• TVS can be augmented with color Doppler.
• Endometrial polyps typically have only one arterial feeding vessel, whereas
submucous leiomyomas generally received blood flow from several vessels
arising from the inner myometrium
Williams gynecology 4th
edition
AUB –A ADENOMYOSIS
Prevalence of adenomyosis varies widely, ranging from 5 % to 70 %
It is defined as growth of endometrial tissue in the myometrium
(beneath the endometrial myometrial junction)
It is difficult to accurately determine the incidence of adenomyosis since the
diagnosis can only be made with certainty by microscopic examination of the
uterus
Gold standard for the diagnosis of adenomyosis - histological examination -
presence of endometrial tissue more than 2.5 mm below the endomyometrial
junction or a junctional zone thickness of more than 12 mm
16.
INVESTIGATIONS
The diagnosiscan be made on the basis of sonographic findings.
The sonographic appearance of adenomyosis is partly related to the absolute
presence of heterotopic endometrial tissue in the myometrium and partly due to the
myometrial hypertrophy.
MUSA – Morphological Uterus Sonographic Assesment group suggest eight
criteria based on transvaginal sonography for the diagnosis of AUB-A Presence
of 2 or more of these diagnostic criteria are highly suggestive of diagnosis of
adenomyosis
FIGO guidelines ., 2018
17.
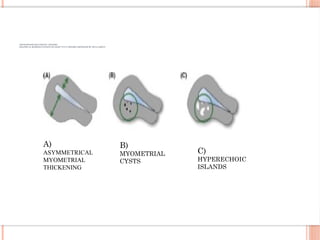
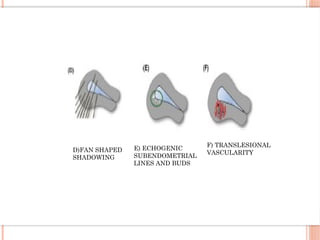
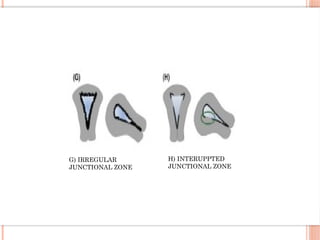
ADENOMYOSIS DIAGNOSTIC CRITERIA
GRAPHICALREPRESENTATIONS OF EIGHT TVUS CRITERIA PROPOSED BY MUSA GROUP
A)
ASYMMETRICAL
MYOMETRIAL
THICKENING
B)
MYOMETRIAL
CYSTS
C)
HYPERECHOIC
ISLANDS
Magnetic Resonance Imaging:
•Gold standard imaging modality for assessing the junctional zone in the
evaluation of adenomyosis
• It clearly distinguishes focal and diffuse adenomyosis from leiomyomatosis.
• The common features on MRI include
– Thickening of the JZ, JZ thickens ≥ 12mm or irregular junctional
thickness with a difference of >5 mm between the maximum &
minimum thickness.
– Islands of ectopic endometrial tissue identified as punctate foci of high signal
intensity on T1 weighted image.
– An ill-defined relatively homogenous low signal intensity (hypoechoic) areas
with scattered high intensity spots in the myometrium on T2 weighted MR
images.
21.
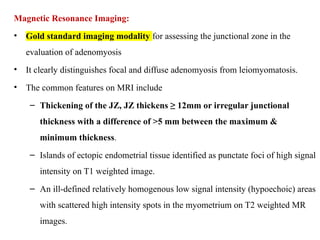
LEIOMYOMA – AUB-L
Most common pelvic tumors
Benign monoclonal tumors arising from
smooth muscle cells of the myometrium that
develop during the reproductive years.
cause AUB, mass abdomen or pelvis,
pelvic pain and infertility
22.
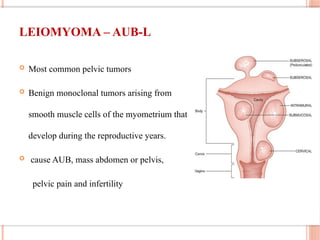
THE THREE STAGECLASSIFICATION
SYSTEM FOR LEIOMYOMA
Primary classification system reflects only
the presence (L1) or absence (L0) of 1 or
more leiomyomas, regardless of the
location, number and size. It requires only
the sonographic confirmation that 1 or
more lesions are present.
In the secondary system, submucous
leiomyomas( SM ) are differentiated from
others (O) because submucosal
leiomyomas are more likely to contribute
to the genesis of AUB.
Tertiary classification system includes the
categorization of the intramural and
subserosal leiomyomas in addition to
category that includes the parasitic
lesions. FIGO guidelines ., 2018
23.
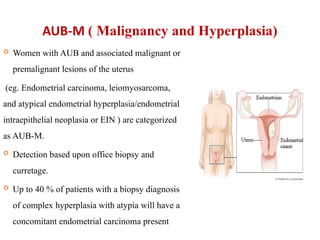
AUB-M ( Malignancyand Hyperplasia)
Women with AUB and associated malignant or
premalignant lesions of the uterus
(eg. Endometrial carcinoma, leiomyosarcoma,
and atypical endometrial hyperplasia/endometrial
intraepithelial neoplasia or EIN ) are categorized
as AUB-M.
Detection based upon office biopsy and
curretage.
Up to 40 % of patients with a biopsy diagnosis
of complex hyperplasia with atypia will have a
concomitant endometrial carcinoma present
24.
AUB- C (COAGULOPATHY )
The term coagulopathy includes the spectrum of systemic disorders of
hemostasis that may be associated with AUB.
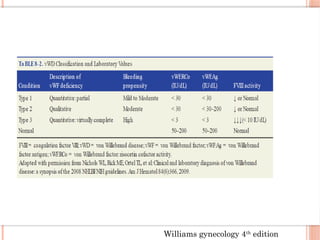
Up to 13% of women with heavy menstrual bleeding have some variant of von
Willebrand disease and up to 20% of women may have an underlying
coagulation disorder (ACOG Practice Bulletin no. 557, 2013)
The onset of heavy menses at menarche is often the first sign of von
willebrand disease (ACOG., 2020)
Etiologies
Von Willebrand’s disease- most common.
Platelet dysfunction
Factor XI deficiency
Factor X deficiency
Women with AUB associated with the use of anticoagulants are now
considered ( FIGO 2018 revision ) iatrogenic and are included in AUB-I
25.
AUB-O ( OVULATORYDYSFUNCTION )
manifest as a combination of unpredictable timing of bleeding and variable
amount of flow
ranges from amenorrhea, through extremely light and infrequent bleeding to
episodes of unpredictable and extreme HMB requiring medical or surgical
intervention.
Etiology-
Polycystic ovarian syndrome, hypothyroidism, hyperprolactinemia, mental
stress, anorexia, obesity, weight loss, or extreme exercise, adolescence,
menopause transition.
FIGO guidelines ., 2018
26.
ANOVULATORY AUB
Responsiblefor 80-90% of AUB
Characterized be irregular cycles, short cycles with scanty flow or amenorrhea
of few months followed by heavy bleeding
It is due to hormonal imbalance and due to alteration of HPO axis
Seen more commonly in adolescents girls, in PCOS, around menopause,
following pregnancy and during lactation
Pathogenesis:
Due to anovulation, there is unopposed estrogenic stimulation of the endometrium,
causing persistent proliferation and hyperplasia of the endometrium, followed by
estrogenic withdrawal bleeding which is painless, irregular and prolonged
Progesterone is responsible for secretion of PGF2a and thromboxane which causes
vasoconstriction
Lack of progesterone is responsible for deficiency of PGF2a and relative increase ion
vasodilator PGE2 and prostacyclin, leads to painless and heavy menstrual bleeding
27.
AUB-E ( ENDOMETRIAL)
When AUB occurs in the context of predictable and cyclic menstrual
bleeding, typical of ovulatory cycles and when no other cause is identified,
the mechanism is probably a disorder of the endometrium. Diagnosed by
EXCLUSION.
Primary disorder of the mechanisms regulating hemostatic mechanisms of the
endometrium.
Deficiency of local production of vasoconstrictors- endothelin-1 and
prostaglandin F 2.
Excessive production of plasminogen activators.
Increased local production of vasodialators- prostaglandin E 2 and
prostacyclin I2
Disorders of the endometrial repair (inflammation)- chlamydial infection.
FIGO guidelines ., 2018
28.
AUB –I (IATROGENIC)
Medical interventions or devices contribute to AUB-I
Medicated or inert intrauterine devices.
Pharmacological agents that directly impact the endometrium, blood coagulation
and systemic control of ovulation.
Gonadal steroid therapy eg, OCPs, cyclic or continuous progesterone ---
break through bleeding.
Cigarette smoking- reduces the level of steroids by enhanced hepatic
metabolism.
Anticonvulsants and antibiotics eg, Rifampicin and Griseofulvin
Systemic agents that interfere with dopamine metabolism eg , Tricyclic
antidepressants ( Amitriptyline and nortriptyline) and phenothiazines.
Use of anticoagulant drugs such as warfarin, heparin and low molecular
weight heparin, rivaroxaban.
FIGO guidelines ., 2018
29.
AUB-N ( NOTOTHERWISE CLASSIFIED)
Disorders that would be identified or defined only by biochemical or
molecular biology assays.
Arterio-venous malformations.
Myometrial hypertrophy.
Chronic endometritis.
Category for new etiologies
FIGO guidelines ., 2018
30.
EVALUATION OF ACASE OF AUB
History
It is important to rule out pregnancy in any woman presenting with AUB
in the reproductive age group.
Other key points include:
Normal cyclicity, amount and duration of menstrual flow prior to onset of
complaints.
Duration of complaint and abnormality one is suffering from.
Associated complaint of pain or lump abdomen, vaginal discharge, fever.
History of use of contraceptives, medicines like anticoagulants, tamoxifen.
History suggestive of thyroid disorder
History of diabetes mellitus, hypertension.
Family history of malignancy.
FOGSI GCPR ., 2016
DETERMINATION OF COAGULATION
DISORDERCONTD.:
This structured history based instrument is 90 % sensitive for the
presence of a coagulopathy in women with the symptom of HMB.
Patients with a positive screening result should be considered for
further evaluation including consultation with a hematologist.
Vwf
Ristocetin CoF
aPTT
PT
Factor VIII
FIGO guidelines ., 2018
FOGSI GCPR ., 2016
33.
EXAMINATION
It isimportant to record the following findings:
Vitals including pulse rate, blood pressure, respiratory rate especially in cases
of acute AUB.
Body Mass Index.
State of pallor, presence of cyanosis, clubbing, icterus, pedal edema and
lymph nodes
Thyroid enlargement.
Acne, hirsutism
Breast examination.
Abdominal examination to look for palpable masses
Speculum examination to look for source and amount of bleeding, nature of
vaginal discharge and state of cervix and vagina. Take PAP smear if indicated.
Vaginal or rectal to confirm the abdominal and speculum findings.
FOGSI GCPR ., 2016
34.
INVESTIGATIONS
Blood Tests
Urine pregnancy test or serum Beta HCG to rule out pregnancy related
event.
Complete blood count including haemoglobin, haematocrit and platelet
count to assess the status of anaemia and coagulability.
Coagulation profile including bleeding time, clotting time, partial
thromboplastin time, activated partial thromboplastin time, von
Willebrand factor assay, ristocetin factor assay and factor VIII activity is
indicated in women with positive screen for coagulopathies in
consultation with a haematologist.
Thyroid stimulating hormone and liver function test if clinically
indicated.
FOGSI GCPR ., 2016
35.
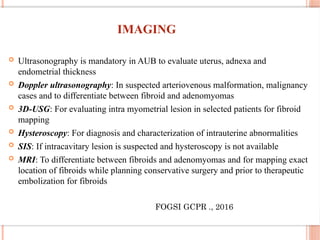
IMAGING
Ultrasonography ismandatory in AUB to evaluate uterus, adnexa and
endometrial thickness
Doppler ultrasonography: In suspected arteriovenous malformation, malignancy
cases and to differentiate between fibroid and adenomyomas
3D-USG: For evaluating intra myometrial lesion in selected patients for fibroid
mapping
Hysteroscopy: For diagnosis and characterization of intrauterine abnormalities
SIS: If intracavitary lesion is suspected and hysteroscopy is not available
MRI: To differentiate between fibroids and adenomyomas and for mapping exact
location of fibroids while planning conservative surgery and prior to therapeutic
embolization for fibroids
FOGSI GCPR ., 2016
36.
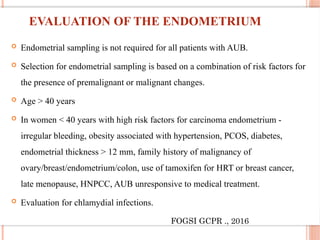
EVALUATION OF THEENDOMETRIUM
Endometrial sampling is not required for all patients with AUB.
Selection for endometrial sampling is based on a combination of risk factors for
the presence of premalignant or malignant changes.
Age > 40 years
In women < 40 years with high risk factors for carcinoma endometrium -
irregular bleeding, obesity associated with hypertension, PCOS, diabetes,
endometrial thickness > 12 mm, family history of malignancy of
ovary/breast/endometrium/colon, use of tamoxifen for HRT or breast cancer,
late menopause, HNPCC, AUB unresponsive to medical treatment.
Evaluation for chlamydial infections.
FOGSI GCPR ., 2016
37.
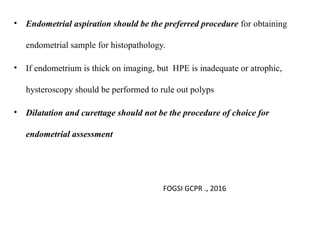
• Endometrial aspirationshould be the preferred procedure for obtaining
endometrial sample for histopathology.
• If endometrium is thick on imaging, but HPE is inadequate or atrophic,
hysteroscopy should be performed to rule out polyps
• Dilatation and curettage should not be the procedure of choice for
endometrial assessment
FOGSI GCPR ., 2016
48
MANAGEMENT
Medical managementshould be initial treatment for most
patients
Need for surgery is based on various factors (stability of
patient, severity of bleed, contraindications to medical
management, underlying cause)
Type of surgery dependent on above + desire for future
fertility
FIGO guidelines ., 2018
CONJUGATED EQUINE ESTROGEN(CEE)
High dose estrogen therapy is useful in controlling acute bleeding episodes
because it promotes rapid endometrial growth to cover denuded endometrial
surface
Stimulating vasospasm of uterine arteries
Promotes platelet aggregation and capillary clotting
Increases fibrinogen, factor V, and factor XI
Increases the production of estrogen and progesterone receptors
Usually used in the intravenous or oral form for acute heavy bleeding
42.
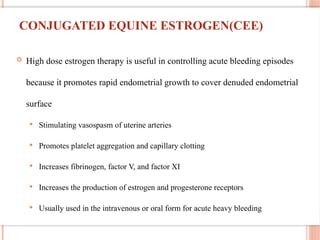
TRANEXAMIC ACID
Thisantifibrinolytic drug
reversibly blocks lysine binding sites
on plasminogen
Normally, plasminogen binds with
tissue plasminogen activator (tPA) to
form plasmin. This binding degrades
fibrin into fibrin degradation products
and leads to clot lysis.
TXA binds to the lysine binding site
on plasminogen. This new
conformation blocks plasmin binding
to fibrin.Fibrin strands are not
broken, and a clot persists to slow
bleeding.
William’s gynecology., 4th
edition
43.
TRANEXAMIC ACID
Approvedby FDA to treat HMB
Reduce MBL by 30-55%
Cost effective when compared with other NSAIDS and when compared with
LNG-IUS
Contra-indication: History of thromboembolism
Dosage:
• 1.3g 3x daily from onset of bleeding up to 5 days
• 10 mg/kg IV every 8 hr in acute AUB
William’s gynecology., 4th
edition
44.
NONSTEROIDALANTI INFLAMMATORY
‐
DRUGS (NSAIDS)
Within the endometrium, cyclooxygenase (COX) converts arachidonic acid
into prostaglandins
NSAIDs reduces prostaglandins synthesis by inhibing COX.
Alter the equilibrium between:
Thromboxane A2 – vasoconstriction/platelet aggregation
Prostacyclin – vasodilation and prevents platelet aggregation
NSAIDs reduce MBL by 25%
NSAIDs are most effective if used with menses onset or just prior to its onset
and continued throughout its duration
Improvement of dysmenorrhea, headache, or nausea are the added benefits.
William’s gynecology., 4th
edition
45.
NONSTEROIDALANTI INFLAMMATORY
‐
DRUGS (NSAIDS)
Patientswith bleeding disorders or platelet function abnormalities should
avoid nonsteroidal antiinflammatory drugs because of their effect on
platelet aggregation and their interaction with drugs that might affect liver
function and the production of clotting factors
William’s gynecology., 4th
edition
46.
PROGESTOGEN ONLY
‐
FORMULATIONS
Commonpreparation used are norethisterone acetate and
medroxyprogesterone acetate
It halts the endometrium growth and allow for an organized sloughing
Inhibits the growth of the endometrium by triggering apoptosis
Inhibits angiogenesis
It stmulates the enzyme (17- beta hydroxy steroid dehydrogenase) that promote
conversion of estradiol to estrone (less potent).
Increases the endometrial ratio of PGF2 alpha / PGE2 and Thromboxane
47.
PROGESTOGEN ONLY FORMULATIONS
‐
Dosingoptions
To stop acute bleeding Norethisterone 5mg tab are used thrice daily till
bleeding stops
Cyclic progesterone therapy –
Typically efficacious for anovulatory bleeding in pubertal and
perimenopausal women,
Medroxyprogesterone 5-10 mg / norethisterone 5-10mg for 21 days
starting from day 5-25 every month for 3-6 cycles
48.
PROGESTOGEN ONLY FORMULATIONS
‐
Continuous progesterone:
Given in those patients who cannot tolerate heavy withdrawal bleeding
and are anaemic
Endometrial hyperplasia does not respond to luteal phase progesterone
hence, treatment with continuous progesterone for 3-6 months is effective
Various continuous preparations may be used. Oral, long acting
intramuscular injections, DMPA implants, progesterone only pills are
effective to reduce menstrual blood loss
DMPA causes endometrial thinning to atrophic levels, which causes
amenorrhea with intermittent spotting (hence not popular)
49.
Mirena IUD/LNG IUDsystem
Release daily doses of 20 micrograms of LNG
Effective for 5 years
Effects:
Prevent endometrial proliferation
Thicken cervical mucus
Suppress ovulation
May be an alternative to hysterectomy in some patients.
Recommended as first line therapy in the absence of any structural or
histological abnormality. (NICE., 2007)
50.
LNG IUD SYSTEM
Contraindications
Abnormal uterine cavity, and reproductive tract infection
Side effects;
BTB in the first cycles, 20% develop amenorrhea within 1 yr
51.
COMBINED ORAL
CONTRACEPTIVES
Usuallya combined oral pills containing 30microgm ethinyl estradiol with
progesterone is given cyclically from 5th
to 25th
day of cycle for 3-6 months
Causes endometrial atrophy, diminished prostaglandin synthesis and decreased
endometrial fibrinolysis
Useful for both ovulatory and anovulatory bleeding
Reduces menstrual volume by about 50%
52.
COMBINED ORAL CONTRACEPTIVES
To stop or slow a heavy period, a “TAPER” can be performed
with any of the low dose monophasic pills.
The treatment begins with 3-4 tablets per day till bleeding
stops, and then gradual tapering to 2 tablets per day for the
next 3 days, and then 1 pill per day until pack is finished and
withdrawal bleeding begins
The patient can be started on one tablet per day of OCPs for next
3-4 cycles or can be started on cyclic progestin therapy if
estrogens are contraindicated
Also treat associated dysmenorrhea and provide added
contraception
Side effects; headache, migraine, weight gain, breast tenderness,
nausea, cholestatic jaundice, hypertension, thrombotic episodes.
53.
ORMELOXIFENE (CENTCHROMAN)
Aselective estrogen receptor modulator usually used as an oral
contraceptive
In AUB dose is 60 mg twice weekly for 3-6 months
54.
GNRH ANALOGUE:
Syntheticpeptide that acts like a natural GnRH but with longer biological half
life.
Cause pituitary down-regulation, severe hypoestrogenism, endometrial atrophy
and amenorrhea
Dose: leuprolide acetate (3.75mg) or goserelin (3.6mg) subcutaneously every
28 days for 3-6 months
Side effects: amenorrhea and menopause like symptoms, (bone loss, hot
flushes and dryness of vagina)
Usually used for short term before surgery
If given for more than 6 months add back therapy should be given such as
estrogen, progesterone or tibolone
Pretreatment with a gonadotrophin-releasing hormone analogue before
hysterectomy and myomectomy should be considered if uterine fibroids are
causing an enlarged or distorted uterus. [NICE, 2007, amended 2020]
55.
ANDROGENS
Danazol
• Aderivative of the synthetic steroid 17α-ethinyl testosterone
• Its net effect creates a hypoestrogenic and hyperandrogenic environment to
induce endometrial atrophy.
• Menstrual loss is reduced by approximately half , and it may even induce
amenorrhea.
Dose: 100 to 200 mg orally daily
Has significant androgenic and hypoestrogenic side effects that include
weight gain, bone loss, oily skin, and acne. Thus, reserved as a second-line drug or
short-term use prior to surgery
William’s gynecology., 4th
edition
56.
MANAGEMENT OF ACUTEAUB
Assess for the signs of hypovolemia & hemodynamic instability
If in hypovolemic shock: Resuscitate with iv fluids and blood transfusion
Blood transfusion is indicated in women with severe anaemia (Hb <7 gm%).
The management strategy is to control the present episode of heavy bleeding and
to reduce menstrual blood loss in subsequent cycles.
ACOG, 2020
MANAGEMENT OF ACUTEAUB
The first-line options in acute AUB include intravenous conjugated estrogen
and oral contraceptive tapers.
If bleeding is not controllled with these agents, additional augmentation
agents may be considered, including tranexamic acid or aminocaproic acid
After immediate stabilization with intravenous conjugated estrogen, patients
should be transitioned to an oral contraceptive taper with the goal to titrate down
eventually to one pill per day.
For the patient who is not a candidate for estrogen therapy, progesterone only
pills can be considered. High-dose progesterone can be delivered orally, with
most pill tapers focusing on norethindrone-acetate, medroxyprogesterone, or
norethindrone alone
ACOG, 2020
59.
MANAGEMENT OF ACUTEAUB
For patients with limited intestinal absorption, injectable depot
medroxyprogesterone acetate (150 mg intramuscularly or 104 mg
subcutaneously) can be administered, with plans for additional backup use of
antifibrinolytics or oral progesterone-only pills
For patients who are anticoagulated, reversal or halting of anticoagulants briefly
in the acute setting to manage heavy bleeding may be necessary and should be
discussed with a hematologist.
Intrauterine insertion of a Foley’s catheter and tamponade by inflating its bulb
with saline has been shown to control the bleeding effectively in select cases.
Once the acute episode of bleeding has been controlled, further treatment of AUB
depends on the aetiology based on the PALM-COEIN classification.
ACOG, 2020
60.
70
CHRONIC TREATMENT
CONSIDERATIONS
• Etiologyand severity of bleeding (eg, anemia, interference with daily
activities)
• Associated symptoms (eg, pelvic pain, infertility)
• Contraceptive needs or plans for future pregnancy
• Contraindications to hormonal or other medications
• Medical co-morbidities
• Patient preferences regarding medical versus surgical and short-term
versus long-term therapy and a careful assessment of risks vs benefits
based on patients medical condition.
61.
MANAGEMENT OF CHRONICAUB
Treatment of anemia is by giving hematinics
Life style modification with weight reduction, diet and exercise in case of
PCOS related AUB
Medical treatment is the mainstay of treatment and should be tried in all
cases of AUB
62.
MANAGEMENT OF AUB-P
Hysteroscopic polypectomy followed by its histopathological examination
(HPE) is the definitive treatment option.
If the HPE report confirms a benign lesion and the patient is not desirous of
fertility, Levonorgestrel- Intrauterine system (LNG-IUS) may be considered.
If the HPE report is suggestive of malignancy, the woman should be managed as
a case of AUB-M.
FOGSI GCPR., 2016
63.
MANAGEMENT OF AUB-A
In women with AUB-A, desirous of preserving fertility but unwilling for
immediate conception, progestogens especially LNG-IUS is recommended as
first-line therapy.
In patients with AUB-A, desirous of preserving fertility and resistant to
LNG-IUS/ unwilling to use LNG-IUS, gonadotropin releasing hormone
(GnRH) agonists with add-back therapy is recommended as second-line
therapy
Combined oral contraceptives, danazol, NSAIDs, and progestogens can be
offered for symptomatic relief where LNG-IUS and GnRH agonists cannot be
indicated
In case of failure/refusal for medical management, vaginal or laparoscopic
hysterectomy FOGSI GCPR., 2016
64.
MANAGEMENT OF AUB-L
Management of fibroid should be individualized depending upon age, parity,
symptoms, fertility desire, size and location of the myoma
Medical management offered for small myoma (<4cm) and to delay or avoid
hysterectomy
Myomectomy is performed for large fibroids causing fertility. It can be
performed by laparoscopy or laparotomy (large fibroids), and by hysteroscopy
(submucous type 0-2, small myoma of <4 cm size)
If family is completed and age is more than 40 years with large symptomatic
fibroids hysterectomy is treatment of choice
65.
MANAGEMENT OF AUB-M
In AUB-M with endometrial malignancy, standard protocol for management of
malignancy should be followed
In AUB-M with endometrial hyperplasia with atypia, hysterectomy is the
standard treatment.
In AUB-M with endometrial hyperplasia without atypia, LNG-IUS can be
considered as first-line therapy; oral progestins can be used if LNG-IUS is
contraindicated or if patient is unwilling for LNG-IUS
FOGSI GCPR., 2016
66.
MANAGEMENT OF AUB-C
Tranexamic acid is the first line treatment (in the dose of maximum 1gm 6
hourly) followed by oral contraceptives or LNG-IUS as a second line therapy.
In cases of persistent heavy bleeding in women with Von-Willebrand disease,
desmopressin can be given in consultation with haematologist.
Recombinant factor VIII, von Willebrand factor or specific factors may also be
required in cases of uncontrolled heavy vaginal bleeding not responding to usual
medical treatments.
NSAIDs are strictly contraindicated in these cases, owing to their adverse
effects on platelets and liver functions.
FOGSI GCPR., 2016
67.
MANAGEMENT OF AUB-O
Oral contraceptives for a total duration of 6-12 months are considered the first
line of therapy
Norethisterone cyclically (for 21 days) is given as initial therapy in acute episodes
of bleeding for short-term management of 3 months.
Cyclical luteal phase progestins are not recommended.
LNG-IUS can also be offered.
The success of any of the available treatment options should be assessed after a
year to evaluate the need to continue or discontinue the treatment or to decide for
hysterectomy.
FOGSI GCPR., 2016
68.
Management of AUB-E(Endometrial):
Similar to the management of AUB-O
Management of AUB-I (Iatrogenic causes):
Whenever possible, medications causing AUB should be changed to other
alternatives, if no alternatives are available, LNG-IUS is recommended
FOGSI GCPR., 2016
69.
MANAGEMENT OF AUB-N
LNG-IUS is recommended as first-line therapy to reduce menstrual bleeding
In patients with AUB-N desirous of continued fertility, in whom, LNG-IUS are
contraindicated, use of COCs are recommended as second line therapy
Non-hormonal options such as NSAIDs and tranexamic acid are recommended
for cyclical AUB.
When medical or conservative surgical treatments (such as ablation) have failed
or are contraindicated, GnRH agonists along with add-back hormone therapy are
recommended, while hysterectomy is suggested as last resort
Uterine Artery embolization is recommended for A-V malformations
FOGSI GCPR., 2016
70.
TREATMENT FOR WOMENWITH NO IDENTIFIED
PATHOLOGY, FIBROID LESS THAN 3 CM IN DIAMETER, OR
SUSPECTED OR DIAGNOSED ADENOMYOSIS
Consider an LNG-IUS as the first line treatment for AUB
If a woman declines an LNG-IUS or is not suitable, consider the following
pharmacologic treatment
Non-hormonal:
Tranexamic acids, NSAIDs
Hormonal:
COCs or cyclical progesterone
NICE Guideline ., 2018
71.
SURGICAL MANAGEMENT OPTIONSFOR
AUB:
Conservative surgery:
Dilation & curettage
Dilatation and curettage was tradionally used earlier for both diagnosis and as a therapeutic
procedure
Used in emergency in HMB for temporary and quick relief of acute bleeding resistant to
hormonal treatment
Do not offer dilatation and curettage as a treatment option for HMB. (NICE guideline .,
2007)
Endometrial ablation and resection techniques
Uterine artery embolization
Myomectomy
72.
ENDOMETRIALABLATION-
This involvesthe dessication of the endometrium’s full thickness along with
superficial layer of the myometrium including the deep basal glands
Indications :
AUB refractory to medical therapy
Young women with AUB who wants to preserve their uterus
Women with AUB at high surgical risk for hysterectomy
73.
ENDOMETRIALABLATION TECHNIQUES:
First generationSecond generation
Performed through hysteroscope under
regional / general anaesthesia
Usually done in the outpatient setting
under local anaesthesia
Transcervical resection of the endometrium Microwave endometrial ablation
Rollerball electrocoagulation Thermal balloon endometrial ablation
Endometrial laser ablation using Nd YAG laser Radiofrequency induced ablation
Cryotherapy, electrode mesh,
interstitial laser
75.
Definitive surgery:
Hysterectomy
Indications of hysterectomy in AUB:
Failure of medical treatment
Failure of conservative surgery
In older women with completed family and severe AUB
76.
MODERN MODALITIES OF
MANAGEMENT
Hysteroscopicapproach:
In modern times hysteroscopy is one of the mainstay in the diagnosis as well
as in treatment of AUB
With the development of miniaturization of instruments (3.5mm or smaller),
safety of distension media and effective local anaesthesia, hysteroscopy is a
fast, effective and much more precise procedure to detect causes of AUB and
plan treatment
NICE guideline recommend outpatient hysteroscopy to women with HMB if
their history suggests submucosal fibroids, polyps or endometrial pathology
(2018)
Appropriate diagnosis and treatment can be provided in an outpatient settings
utilizing a one stop approach. It includes combination of key history taking,
examination, TVS and hysteroscopy, if indicated at the same visit.
77.
MODERN MODALITIES OFMANAGEMENT:
RADIOLOGICAL INTERVENTIONS:
Uterine Artery Embolization (UAE)
An angiographic interventional procedure in which polyvinyl alcohol particles or
other synthetic particulate emboli are delivered into both uterine arteries
obstructing blood flow in uterine arteries to produce ischaemia and necrosis of
myoma and adenomyoma
MRI Guided High Intensity Focussed Ultrasound
Under MRI , high intensity ultrasound energy is focussed on the myoma to
produce heat causing coagulative necrosis
Indicated in myoma of size ranging from 3cm to 10 cm
A 3 hour long session may be required to treat a fibroid of approx 7-8 cm size
78.
SUMMARY
AUB iscommon among women worlwide
A detailed history is an important first step in evaluating a women who
presents with AUB
The etiologies of AUB should be classified based on the PALM–COEIN
system
Treatment is based on etiology, desire for future fertility and medical
morbidities
Medical management should be the initial treatment for most patients, if
clinically appropriate.
The need for surgical treatment is based on the clinical stability of the patient,
the severity of bleeding, contraindications to medical management, the
patient’s lack of response to medical management, and the underlying medical
condition of the patient.
1. In premenarchalgirls, which of the following is the
most common source of bleeding
Ovary
Uterus
Vagina
Urethra
81.
1. In premenarchalgirls, which of the following is the
most common source of bleeding
Ovary
Uterus
Vagina
Urethra
82.
2. Which layerof the endometrium sloughs and therefore is
responsible for menstrual bleeding
Spiral
Radial
Basalis
Functionalis
83.
2..Which layerof the endometrium sloughs and therefore
is responsible for menstrual bleeding
Spiral
Radial
Basalis
Functionalis
84.
3.Control ofblood loss during menses involves which of
the following mechanisms
Thrombus formation
Platelet aggregation
Vasoconstriction of endometrial arteries
All of the above
85.
3..Control ofblood loss during menses involves which of
the following mechanisms
Thrombus formation
Platelet aggregation
Vasoconstriction of endometrial arteries
All of the above
86.
4..According toFIGO 2018 , endometrial sampling to
assess AUB in NOT recommended for a women with
which of the following characteristics
Is 35 years old
Has failed medical management
Has persistent abnormal uterine bleeding
Has history of unopposed estrogen exposure
87.
4..According toFIGO 2018 , endometrial sampling to
assess AUB in NOT recommended for a women with
which of the following characteristics
Is 35 years old
Has failed medical management
Has persistent abnormal uterine bleeding
Has history of unopposed estrogen exposure
Answer: ≥ 45 years old
88.
5..Which causeof AUB is NOT represented in the
FIGO, 2018 classification acronym PALM-COIEN
Leiomyoma
Malignancy
Iatrogenic
Not yet classified
89.
5..Which causeof AUB is NOT represented in the
FIGO, 2018 classification acronym PALM-COIEN
Leiomyoma
Malignancy
Iatrogenic
Not yet classified
Answer : N stands for Not otherwise classified
90.
6..A patientpresent to the emergency department with a 1 day history of heavy
vaginal bleeding . She is tachycardic but not hypotensive and vitals are stable.
Physical examination reveals bleeding from the external cervical os and continued
pooling of blood in the vagina. Laboratory studies reveal she is anaemic. which of
the following is the most appropriate first line agent to attempt control of her acute
uterine bleeding
Iv estrogen
Oral tranexamic acid
GnRH agonist
COCs taper
91.
6..A patientpresent to the emergency department with a 1 day history of heavy
vaginal bleeding . She is tachycardic but not hypotensive and vitals are stable.
Physical examination reveals bleeding from the external cervical os and continued
pooling of blood in the vagina. Laboratory studies reveal she is anaemic. which of
the following is the most appropriate first line agent to attempt control of her acute
uterine bleeding
Iv estrogen
Oral tranexamic acid
GnRH agonist
COCs taper



![GNRH ANALOGUE:
Synthetic peptide that acts like a natural GnRH but with longer biological half
life.
Cause pituitary down-regulation, severe hypoestrogenism, endometrial atrophy
and amenorrhea
Dose: leuprolide acetate (3.75mg) or goserelin (3.6mg) subcutaneously every
28 days for 3-6 months
Side effects: amenorrhea and menopause like symptoms, (bone loss, hot
flushes and dryness of vagina)
Usually used for short term before surgery
If given for more than 6 months add back therapy should be given such as
estrogen, progesterone or tibolone
Pretreatment with a gonadotrophin-releasing hormone analogue before
hysterectomy and myomectomy should be considered if uterine fibroids are
causing an enlarged or distorted uterus. [NICE, 2007, amended 2020]](https://image.slidesharecdn.com/abnormaluterinebleeding-251109111339-ccc78a41/85/Abnormal-Uterine-Bleeding-aiims-patna-gyn-54-320.jpg)






























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















