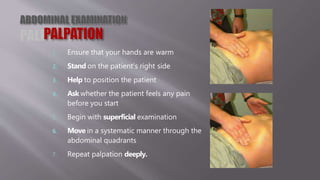
1. The document provides guidance on performing an abdominal examination, including ensuring warm hands, standing at the patient's right side, and palpating the abdomen in a systematic manner across quadrants.
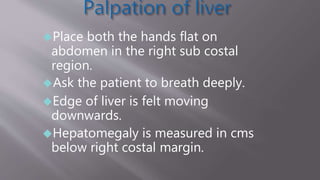
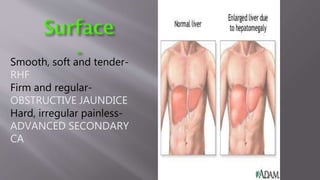
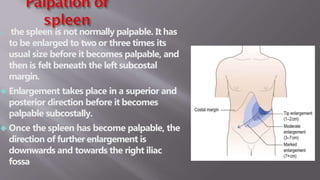
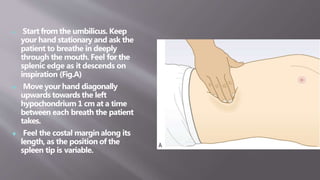
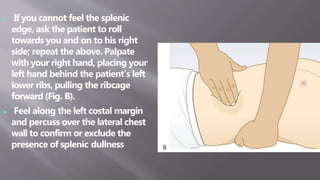
2. Specific examination techniques are described for assessing the liver, gallbladder, spleen, and lymph nodes, including how to feel for organ edges and changes related to common conditions.
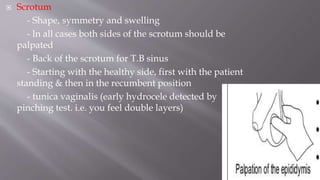
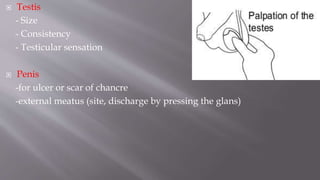
3. The genital and hernia examinations are also summarized, outlining what to inspect for the scrotum, testes, penis, and location of any tenderness.