Download as PDF, PPTX


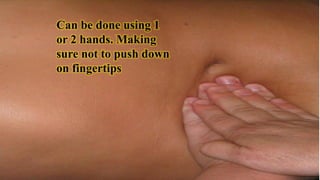

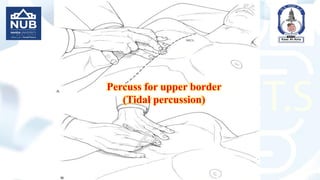



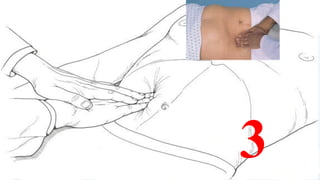
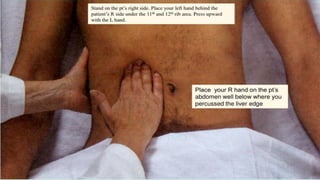
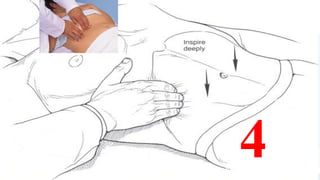

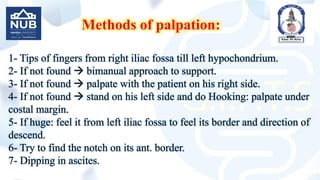




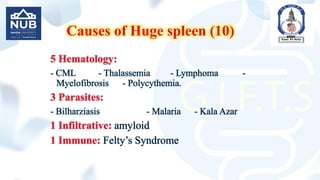


This document provides guidance on performing an abdominal examination through inspection, palpation, percussion, and auscultation. It describes the techniques for superficial and deep palpation of the abdomen while assessing for organomegaly. Specific instructions are given for palpating the liver and spleen, including common examination methods to determine size, edge, consistency, surface, tenderness, and pulsation. Causes of apparent or tender hepatomegaly and huge splenomegaly are also listed.
![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)


































































