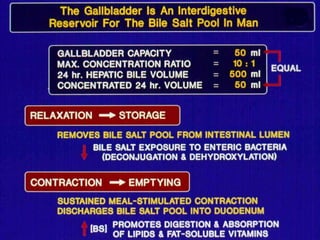
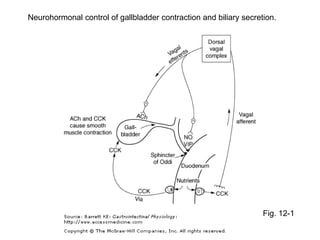
The document covers the functions and anatomy of the liver, detailing its roles in metabolism, detoxification, bile production, and ammonia regulation. It also discusses the gallbladder's function in bile storage and concentration, as well as gallstone disease and its treatment options. Additionally, enterohepatic circulation is highlighted as a key process for bile salt recycling.