Movement of BodyFluids: Important Concept
3
• Body fluids are not static. Fluids & electrolytes
shift from compartment to compartment.
• Emphasis is always on maintaining homeostasis
Homeostasis
5
Central conceptof physiology
Physiological systems have evolved to maintain
their internal environment while responding to
both internal and external threats to that stability.
Disease, by and large, is a failure of homeostasis
Excessive perturbations result ultimately in death of the
organism.
6.
Homeostasis
6
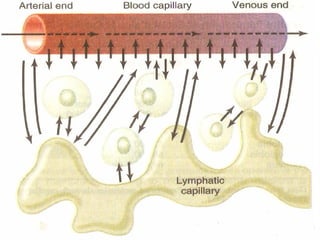
The internalenvironment of the body is tissue
fluid, which bathes all cells making up the body.
The composition of tissue fluid must remain
constant if cells are to remain alive and healthy.
Tissue fluid is nourished and purified when
molecules are exchanged across thin capillary
walls.
Tissue fluid remains constant only if the
composition of blood remains constant.
7.
7
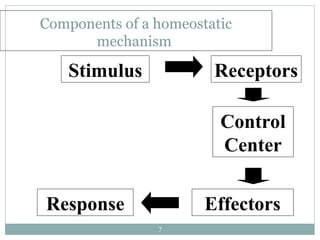
Components of ahomeostatic
mechanism
Stimulus Receptors
Control
Center
Effectors
Response
8.
Maintaining Homeostasis
8
Regulationof homeostasis of body fluids- kidneys,
endocrine system, CV, lungs, GI system.
Hormones - antidiuretic hormone (ADH), renin-
angiontensin-aldosterone system, atrial natriuretic
factor.
9.
9
Fluid compartmentsare separated by membranes that are
freely permeable to water.
Movement of fluids due to STARLING FORCES :
1. Capillary hydrostatic pressure---tends to move fluid
outward from capillaries to interstitial spaces
2. Capillary colloid osmotic pressure-----(plasma
proteins) fluid movement inward from interstitial spaces to
capillaries
10.
10
03. Interstitial hydrostaticpressure----fluid movement
inward from interstitial spaces to capillaries
04. Tissue colloid osmotic pressure----- tends to move
fluid outward from capillaries to interstitial spaces
12
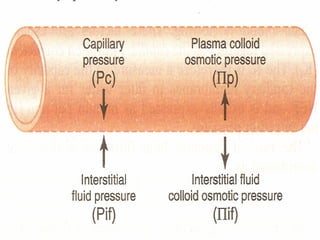
• the sumof Starling forces usually drives the movement of
water and solutes from interstitium into capillary.
• In favor of moving things from interstitium into capillaries are:
capillary colloid osmotic pressure (Pcap
)
interstitial hydrostatic pressure (PIS
)
• The opposing forces are:
interstitial colloid osmotic pressure (PIS
)
capillary hydrostatic pressure (Pcap
).
13.
13
CLINICAL SIGNIFICANCE:
Edema isthe accumulation of fluid within the
interstitial spaces.
Causes:
increased capillary hydrostatic pressure
decreased capillary colloid osmotic pressure
increased capillary membrane permeability
14.
14
Increases Capillary Hydrostaticpressure :
Venous obstruction:
Thrombophlebitis (inflammation of veins)
hepatic obstruction
tight clothing on extremities
prolonged standing
Salt or water retention
congestive heart failure
renal failure
15.
15
Decreased Capillary colloidosmotic
pressure:
↓ plasma albumin (liver disease or
protein malnutrition)
plasma proteins lost in :
glomerular diseases of kidney
hemorrhage, burns, open wounds
“ WHERE SODIUMGOES, WATER FOLLOWS.”
DIFFUSION – MOVEMENT OF PARTICLES DOWN A CONCENTRATION
GRADIENT.
OSMOSIS – DIFFUSION OF WATER ACROSS A SELECTIVELY PERMEABLE
MEMBRANE
ACTIVE TRANSPORT – MOVEMENT OF PARTICLES UP A CONCENTRATION
GRADIENT ; REQUIRES ENERGY
17
FLUID MOVEMENT:
18.
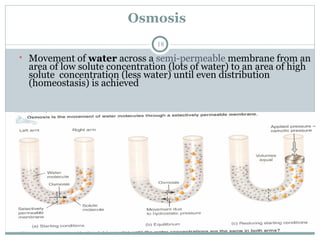
Osmosis
18
• Movement ofwater across a semi-permeable membrane from an
area of low solute concentration (lots of water) to an area of high
solute concentration (less water) until even distribution
(homeostasis) is achieved
19.
selectively permeable membrane
19
A membrane that allows only certain materials to
cross it
Materials pass through pores in the membrane
Osmotic pressure: Pressure required to prevent
osmosis
20.
20
Osmolarity =number of solute particles (milli-
osmoles) in liter of solution
Normal = 270 – 300 (or 275 – 295) mOsm/l
Osmolality = number of solute particles (mill-
osmoles) in kilogram of water
mOsm (milliosmoles) = number of particles
in a solution
22
Tonicity of asolution :
Is the effect of solution on the cell volume
determined by conc. of non penetrating
solutes.
Solutes that can penetrate plasma membrane
distribute equally b/w ECF & ICF- do not
contribute to osmotic differences.
Isotonic – same conc. of solutes as body fluids.
Hypertonic – above normal conc.
Hypotonic – below normal.
23.
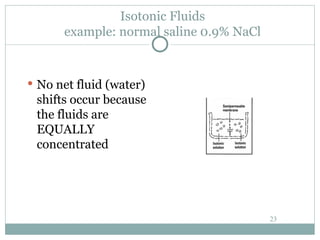
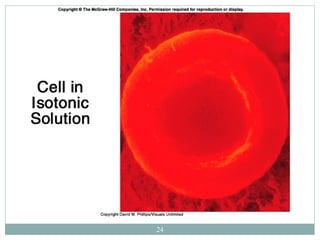
Isotonic Fluids
example: normalsaline 0.9% NaCl
No net fluid (water)
shifts occur because
the fluids are
EQUALLY
concentrated
23
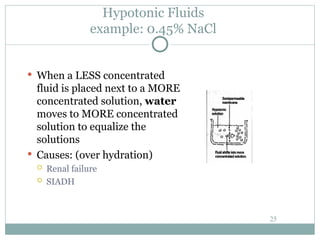
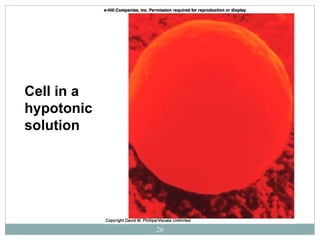
Hypotonic Fluids
example: 0.45%NaCl
When a LESS concentrated
fluid is placed next to a MORE
concentrated solution, water
moves to MORE concentrated
solution to equalize the
solutions
Causes: (over hydration)
Renal failure
SIADH
25
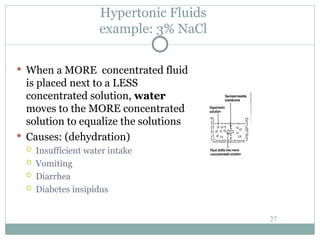
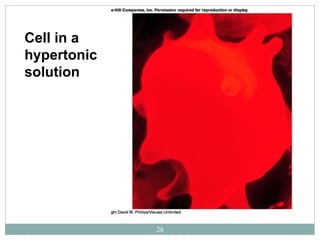
Hypertonic Fluids
example: 3%NaCl
When a MORE concentrated fluid
is placed next to a LESS
concentrated solution, water
moves to the MORE concentrated
solution to equalize the solutions
Causes: (dehydration)
Insufficient water intake
Vomiting
Diarrhea
Diabetes insipidus
27
WATER BALANCE
29
NORMAL WATERCONTENT OF BODY
75% AT BIRTH
55-60% YOUNG ADULTS
MEN SLIGHTLY HIGHER THAN WOMEN
(MORE FAT, LESS WATER)
45% IN ELDERLY, OBESE
30.
WATER BALANCE
30
TOTAL BODYWATER
~40 liters
Fluid compartments
65% (25L)INTRACELLULAR FLUID (ICF)
35% (15L)EXTRACELLULAR FLUID (ECF)
25% interstitial fluid (tissue fluid)---------
8% blood plasma and lymph-------
2% transcellular fluid--------
31.
31
Interstitial fluid(tissue fluid)---Fluid b/w the cells
Plasma------noncelluler part of blood
Lymph-------colorless liquid
Transcellular fluid--------
synovia,pericardial,peritoneal,plural,inttaocular, CFS.
32.
32
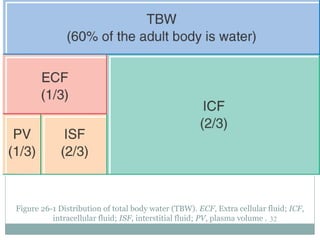
Figure 26-1 Distributionof total body water (TBW). ECF, Extra cellular fluid; ICF,
intracellular fluid; ISF, interstitial fluid; PV, plasma volume .
33.
33
Balance
Fluid andelectrolyte homeostasis is maintained
in the body
Neutral balance: input = output
Positive balance: input > output
Negative balance: input < output
34.
Body Fluid Regulation
34
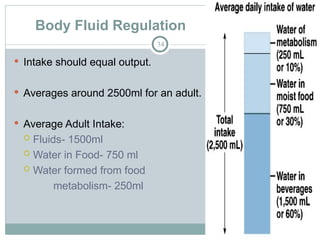
Intake should equal output.
Averages around 2500ml for an adult.
Average Adult Intake:
Fluids- 1500ml
Water in Food- 750 ml
Water formed from food
metabolism- 250ml
ELECTROLYTES
36
Substance whendissolved in solution separates
into ions & carry an electrical charge
CAT ION - positively charged electrolyte
AN ION - negatively charged electrolyte
# Cat ions must = # Anions for homeostasis
is to exist in each fluid compartment
Commonly measured in mill equivalents / liter
(mEq/L)
Extracellular and IntracellularFluids
38
Each fluid compartment of the body has a distinctive
pattern of electrolytes
Interstitial fluids are similar plasma (except for the
high protein)
Sodium is the chief cation
Chloride is the major anion
Intracellular fluids have low sodium and chloride
Potassium is the chief cation
Phosphate is the chief anion
39.
Extracellular and IntracellularFluids
39
Sodium and potassium concentrations in extra and
intracellular fluids are nearly opposites
This reflects the activity of cellular ATP-dependent
sodium-potassium pumps
Electrolytes determine the chemical and physical
reactions of fluids
40.
Electrolyte Regulation
40
Mostelectrolytes come from dietary intake and
excreted by urine.
Na+ & Cl- not stored-must be consumed daily.
K+ & Ca+ are stored in cells and bones.
When serum levels drop, ions can go from storage
into blood to maintain adequate serum levels.
41.
Sodium: Na+: 135-145mEq/L
41
Major ECF cat ion
Major functions:
Water balance
Transmission of nerve impulses
Regulation controlled at cellular level by sodium-
potassium pump.
Na+ retention/secretion controlled by aldosterone
Aldosterone controlled by renin-angiotensin
42.
Potassium: K+: 3.5-5.5mEq/L
42
Major cation of ICF
Major function: Electrical conduction of nerve impulses-
cardiac conduction
Regulation at cellular level by Na-K pump
Body more sensitive to small changes in serum K+ than
other electrolytes
43.
Calcium: Ca++: 8.5-10.5mg/dl
43
• Major functions: 1% in ECF
– Normal skeletal muscle, smooth muscle, & cardiac
muscle contraction; blood clotting
• Taken through diet. Needs Vit. D. to be absorbed
• Regulation:
– Parathyroid hormone: triggers Ca release from bone
and/or inhibits renal excretion: raises serum levels
– Calcitonin: thyroid gland; causes ECF levels to decrease
by inhibition of bone resorption (release); inhibits Vit. D
absorption, & increases renal excretion
44.
Chloride: Cl-
44
Majoran ion of ECF
Functions with Na to regulate serum osmolality and
blood volume
Major component of gastric juice (HCl).
Helps regulate acid-base balance.
Acts as buffer in exchange of O2 & CO2 in RBC’s.
45.
REGULATION OF NaCl& WATER
REABSORPTION
45
Most important factors:
Angiotensin II
Aldosterone: Controls Na+
absorption and K+
loss through kidney
ADH: Stimulates water conservation
ANP : Reduce thirst and block the release of ADH and aldosterone
Sympathetic nerves
Other factors:
Dopamine
Glucocorticoids
Starling forces & the phenomenon of
glomerulotubular balance.
46.
46
• ANGIOTENSIN II:
•a potent stimulator of NaCl & water reabsorption from
kidney
• Stimulates aldosterone
• The reduction in extracellular fluid volume activates
RENIN-ANGIOTENSIN system which leads to
increased plasma angiotensin II concentration.
49
Patients ofCongestive Heart Failure /
Hypertension
treated with angiotensin-converting enzyme (ACE)
inhibitors (e.g., captopril) to lower ECFV & BP
Inhibition of ACE lowers the convesrion of
angiotensin I to II
lowers plasma [angiotensin II]
50.
50
ALDOSTERONE:
Synthesizedin adrenal cortex
Stimulates NaCl reabsorption in distal tubule / collecting duct
As well as from :
gut
sweat glands
salivary glands
Also increases water reabsorption in collecting duct secondary to the
increased NaCl reabsorption
Stimulates K+ secretion in distal tubule / collecting duct
The two most important stimuli for aldosterone secretion: increased
plasma ANGIOTENSIN II & increased plasma K+
51.
51
Atrial Natriuretic Peptide(ANP):
Is secreted by cells of atria / kidney
Secretion is stimulated by increased BP & by
increased ECFV
Increases urinary NaCl excretion
also increases urinary water excretion by directly
inhibiting water reabsorption in collecting duct & by
inhibiting ADH secretion
52.
52
Antidiuretic Hormone(ADH):
Is the most important hormone that regulates water
balance
ADH is secreted by posterior pituitary in response to
increased plasma osmolality or decreased ECFV
ADH increases water permeability in COLLECTING
DUCT, thus conserving body water
ADH DOES NOT AFFECT URINARY NaCl
EXCRETION
53.
ADH Disturbances
53
DiabetesInsipidus (dec ADH)
Posterior pituitary (central) / kidney (nephrogenic)
Loss of 15 liters of fluid per day
Treatment: Vasopressin and fluid replacement
Syndrome of Inappropriate Anti-Diuretic Hormone (SIADH)
(inc ADH)
Fluid retention (excess)
Hyponatremia
Treatment: Diuretics and fluid restriction
54.
54
Sympathetic Nerves:
( activationcaused by hemorrhage or decreased
ECFV)
Catecholamines released from sympathetic nerves
(norepinephrine) & adrenal medulla (epinephrine)
stimulate NaCl & water reabsorption in proximal
tubule & thick ascending limb of Henle’s loop
55.
55
2 Rules ofElectrolyte Balance
1. Most common problems with electrolyte
balance are caused by imbalance between
gains and losses of sodium ions
2. Problems with potassium balance are less
common, but more dangerous than sodium
imbalance
56.
Common Disturbances ElectrolyteBalance
56
Hypernatremia (high levels of sodium)
(Na > 145)
Caused by excess water loss or overall sodium excess
Water moves from ICF ECF
→
Cells dehydrate
Causes:
excess salt intake,
hypertonic solutions,
excess aldosterone,
diabetes – polyuria,
increased water loss - long term sweating with chronic fever,
water deprivation (hypodipsia)
Hypernatremia - Clinicalmanifestations
58
Thirst
Dry & flushed skin
Dry & sticky tongue and mucous membranes
Lethargy
Neurological dysfunction due to dehydration of brain
cells
Decreased vascular volume
59.
Hypernatremia - Labfindings
59
high serum sodium > 145mEq/L
high serum osmolality > 295mOsm/kg
high urine specificity > 1.030
60.
60
Hypernatremia - Management
Lower serum Na+
Administration of hypotonic sodium solution [0.3 or 0.45%]
Rapid lowering of sodium can cause cerebral edema
Slow administration of IV fluids with the goal of reducing sodium not
more than 08 to 10 mEq/L for the first 48 hrs decreases this risk
In case of Diabetes insipidus desmopressin acetate nasal spray is used
Dietary restriction of sodium in high risk clients
60
61.
Hyponatremia (Na <135)
61
Overall decrease in Na+ in ECF
Occurs with net loss of sodium or net water excess
Causes:
diuretics
chronic vomiting
chronic diarrhea
decreased aldosterone
decreased Na+ intake
increased sweating
SIADH
Hyponatremia – Labfindings
63
Serum sodium less than 135mEq/ L
serum osmolality less than 280mOsm/kg
urine specific gravity less than 1.010
64.
Hyponatremia - management
64
Identify the cause and treat
Administration of sodium orally, by NG tube or
parenterally
For patients who are able to eat & drink, sodium is easily
accomplished through normal diet
For those unable to eat, Ringer’s lactate solution or isotonic
saline [0.9%Nacl]is given
For very low sodium 3%Nacl may be indicated
water restriction in case of hypervolaemia
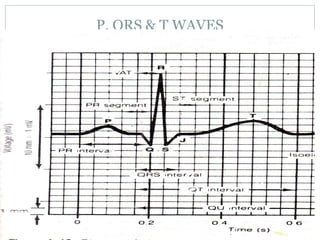
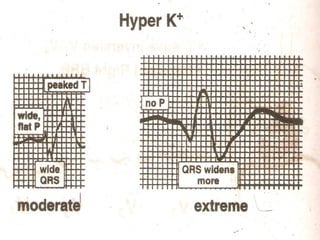
Hyperkalemia - Labfindings
67
serum potassium of 5.3mEq/L results in peaked T
wave HR 60 to 110
serum potassium of 7mEq/L results in low broad P-
wave
serum potassium levels of 8mEq/L results in no
arterial activity[no p-wave]
70
Hyperkalemia- management
Dietaryrestriction of potassium for potassium
Mild hyperkalemia can be corrected by improving output
by forcing fluids, giving IV saline or potassium wasting
diuretics
Severe hyperkalemia is managed by
1.infusion of calcium gluconate to decrease the antagonistic effect
of potassium excess on myocardium
2.infusion of insulin and glucose or sodium bicarbonate to
promote potassium uptake
3.sodium polystyrene sulfonate [Kayexalate] given orally or
rectally as retention enema
71.
71
Hypokalemia decrease potassium
Serum K+
< 3.5 mEq /L
Beware if diabetic
Insulin gets K+
into cell
Ketoacidosis – H+
replaces K+
, which is lost in urine
β – adrenergic drugs or epinephrine
71
72.
72
Causes of Hypokalemia
Decreased intake of K+
Increased K+
loss
Chronic diuretics
Acid/base imbalance
Trauma and stress
Increased aldosterone
Redistribution between ICF and ECF
72
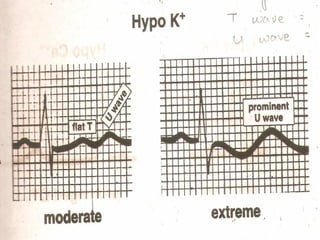
Hypokalemia - Labfindings
74
K – less than 3mEq/L results in ST depression , flat
T wave, taller U wave
K – less than 2mEq/L cause widened QRS,
depressed ST, inverted T wave
Hypokalemia - Management
76
Mild hypokalemia[3.3to 3.5] can be managed by
oral potassium replacement
Moderate hypokalemia
K-3.0to 3.4mEq/L need 100to 200mEq/L of IV
potassium for the level to rise to 1mEq/L
Severe hypokalemia K- less than 3.0mEq/L
need 200to 400 mEq/L for the level to rise to l
mEq/L
Dietary replacement of potassium helps in
correcting the problem[1875 to 5625 mg/day]
77.
77
Calcium Imbalances
Mostin ECF
Regulated by:
Parathyroid hormone
↑Blood Ca++
by stimulating osteoclasts
↑GI absorption and renal retention
Calcitonin from the thyroid gland
Promotes bone formation
↑ renal excretion
78.
78
Hypercalcemia
calcium plasmalevel over 11mg/dl
Causes:
Hyperparathyroidism
Hypothyroid states
Renal disease
Excessive intake of vitamin D
Milk-alkali syndrome
Certain drugs
Malignant tumors
78
79.
79
Hypercalcemia – Clinicalmanifestations
Many nonspecific – fatigue, weakness, lethargy
Increases formation of kidney stones and pancreatic stones
Muscle cramps
Bradycardia, cardiac arrest
Pain
GI activity also common
Nausea, abdominal cramps
Diarrhea / constipation
Decreased level of consciousness
79
80.
Hypercalcemia - Labfindings
80
High serum calcium level 11mg/dl,
x- ray showing generalized osteoporosis,
widened bone cavitation,
urinary stones,
elevated BUN 25mg/100ml,
elevated creatinine1.5mg/100ml
81.
Hypercalcemia - Management
81
1.IV normal saline, given rapidly with Lasix promotes
urinary excretion of calcium
2.Plicamycin an antitumor antibiotics decrease the plasma
calcium level
3.Calcitonin decreases serum calcium level
4.Corticosteroid drugs compete with vitamin D and
decreases intestinal absorption of calcium
5. If cause is excessive use of calcium or vitamin D
supplements reduce or avoid the same
82.
82
Hypocalcaemia
It isa plasma calcium level below 8.5 mg/dl
Hyperactive neuromuscular reflexes and tetany differentiate it
from hypercalcemia
Convulsions in severe cases
Caused by:
Renal failure
Lack of vitamin D
Suppression of parathyroid function
Hypersecretion of calcitonin
Malabsorption states
Abnormal intestinal acidity and acid/ base bal.
Widespread infection or peritoneal inflammation
82
83.
83
Hypocalcemia - Clinicalmanifestation
Numbness and tingling sensation of fingers,
hyperactive reflexes,
muscle cramps,
pathological fractures,
prolonged bleeding time
83
Hypocalcemia - Management
85
1.Asymtomatic hypocalcemia is treated with oral
calcium chloride, calcium gluconate or calcium
lactate
2.Tetany from acute hypocalcemia needs IV
calcium chloride or calcium gluconate to avoid
hypotension bradycardia and other dysrythmias
3.Chronic or mild hypocalcemia can be treated by
consumption of food high in calcium
86.
Volume Regulation
86
Sincethe osmolarity (i.e. concentration) of ECF is
tightly controlled,
the volume of the ECF is determined by the total
quantity of solute (mainly NaCl),
so regulation of ECF volume is all about Sodium
Balance
87.
FLIUD IMBALANCES
87
The fivetypes of fluid imbalances that may
occur are:
Extracellular fluid Volume deficit (EVFVD)
Extracellular fluid volume excess(ECFVE)
Extracellular fluid volume shift
Intracellular fluid volume excess(ICFVE)
Intracellular fluid volume deficit(ICFVD)
88.
EXTRACELULLAR FLUID VOLUMEDEFICIT
88
An ECFVD, commonly called as dehydration , is
a decrease in intravascular and interstitial fluids
An ECFVD can result in cellular fluid loss if it is
sudden or severe
89.
THREE TYPES OFECFVD
89
Hyperosmolar fluid volume deficit- water loss is
greater than the electrolyte loss
Isosmolar fluid volume deficit – equal proportion of
fluid and electrolyte loss
Hypotonic fluid volume deficit – electrolyte loss is
greater than fluid loss
90.
ETIOLOGY AND RISKFACTORS
90
Severe vomiting.
Diaphoresis.
Traumatic injuries.
Third space fluid shifts
[percardial, pleural,
peritoneal and joint
cavities]
Fever.
Gastrointestinal suction.
Ileostomy.
Fistulas.
Burns.
Hyperventilation.
Decreased ADH
secretions.
Diabetes insipidus.
Addison’s disease or
adrenal crisis.
Diuretic phase of acute
renal failure.
Use of diuretics.
91.
CLINICAL MANIFESTATION
91
InMild ECFVD, 1to 2 L of water or 2% of the body
weight is lost
In Moderate ECFVD, 3 to 5L of water loss or
5%weight loss
IN Severe ECFVD , 5 to 10 L of water loss or 8% of
weight loss
92.
CLINICAL MANIFESTATION
92
Thirst
Muscle weakness
Dry mucus
Eyeballs soft and sunken
(severe deficit)
Apprehension ,
restlessness, headache ,
confusion, coma in
severe deficit
Elevated temperature
Tachycardia, weak
thready pulse
Peripheral vein filling> 5
seconds
Postural systolic BP falls
>25mm Hg and diastolic
fall > 20 mm Hg , with
pulse increases > 30
Narrowed pulse pressure,
decreased CVP.
Flattened neck veins in
supine position
Weight loss
Oliguria(< 30 mlper hour)
93.
LABORATORY FINDINGS
93
Increasedosmolality(> 295 mOsm/ kg)
Increased or normal serum sodium level (> 145mEq/
L )
Increase BUN (>25 mg / L )
Hyperglycemia ( >120 mg /dl )
Elevated hematocrit (> 55%)
Increased specific gravity ( > 1.030)
94.
MANAGEMENT
94
Mild fluid volumeloss can be corrected with oral fluid
replacement
-if client tolerates solid foods advice to take 1200 ml to
1500ml of oral fluids
-if client takes only fluids, increase the total intake to
2500 ml in 24 hours
95.
Management of Hyperosmolarfluid volume
deficit
95
Administration of hypotonic IV solution , such as 5%
dextrose in 0.2 %saline
If the deficit has existed for more than 24
hours,avoid rapid correction of fluid [sodium
solution to be infused at the rate of 0.5 to 0.1m Eq/
L/ hr]
96.
If heamorrhage isthe cause for ECFVD
96
Packed red cells followed by hypotonic IV fluids is
administered
In situations where the blood loss is less than 1 L
normal saline or ringer lactate may be used
clients with severe ECFVD accompanied by severe
heart , liver, or kidney disease cannot tolerate large
volumes of fluid and sodium
97.
EXTRACELLULAR FLUID VOLUMEEXCESS
97
ECFVE is increased fluid retention in the
intravascular and interstitial spaces (edema)
98.
ETIOLOGY AND RISKFACTORS
98
Heart failure
Renal disorders
Cirrhosis of liver
Increased ingestion of high sodium foods
Excessive amount of IV fluids containing sodium
Electrolyte free IV fluids
SIADH,Sepsis
decreased colloid osmotic pressure
lymphatic and venous obstruction
Cushing’s syndrome & glucocorticoids
99.
CLINICAL MANIFESTATION
99
Constantirritating cough
Dyspnea & crackles in lungs
Cyanosis, pleural effusion
Neck vein obstruction
Bounding pulse &elevated BP
S3 gallop
Pitting & sacral edema
Weight gain
Change in level of consciousness
100.
LAB INVESTIGATION
100
serumosmolality <275mOsm/ kg
Low , normal or high sodium
Decreased hematocrit [ < 45%]
Specific gravity below 1.010
Decreased BUN [< 8mg/ dl]
101.
MANAGEMENT
101
Diuretics [combinationof potassium sparing and
potassium depleting diuretics]
In people with CHF, ACE inhibitors and low dose of
beta blockers are used
A low sodium diet
102.
EXTRACELLULAR FLUID VOLUMESHIFT:
THIRD SPACING
102
Fluid that shifts into the interstitial spaces and
remain there is called as third space fluid
Common sites are abdomen , pleural cavity,
peritoneal cavity and pericardial sac
103.
RISK FACTORS
103
• Crushinginjuries, major tissue trauma
• Major surgery
• Extensive burns
• Acid –base imbalances and sepsis
• Perforated peptic ulcers
• Intestinal obstruction
• Lymphatic obstruction
• Autoimmune disorders
• Hypoalbunemia
• GI tract malabsorption
104.
CLINICAL MANIFESTATION
104
skinpallor
Cold extremities
Weak and rapid pulse
Hypotension
Oliguria
Decreased levels of consciousness
LAB INVESTIGATION
Elevated hematocrit & BUN level
105.
MANAGEMENT
105
Treat the cause
1.For burns and tissue injuries large volume of
isosmolar IV fluid is administered
2. Albumin is administered for protein deficit
3. IV fluid intake is maintained after major surgery
to maintain kidney perfusion
4. Pericardiocentesis if pericarditis is the result
5. Paracentesis for ascitis
ETIOLOGY
107
Administration ofexcessive amount of hyposmolar
IV fluids[0.45%saline or 5%dextrose in water]
Consumption of excessive amount of tap water
without adequate nutritional intake
SIADH
Schizophrenia[compulsive water consumption]
108.
CLINICAL MANIFESTATIONS
108
Headaches
Behavioral changes
Apprehension
Irritability, disorientation and confusion
Increased ICP – papillary changes and decreased
motor and sensory function
Bradycardia, elevated BP, widened pulse pressure
& altered respiratory patterns, Babinski’s response
flaccidity, projectile vomiting, Papilledema,
delirium, convulsions &coma
MANAGEMENT
110
Early administrationof IV fluids containing
sodium chloride cam prevent SIADH
oral fluids such as juices or soft drinks can be given
orally every hour
Perform neurologic checks every hour to see if
cranial changes are present
Monitor fluid intake , IV fluids and fluid output
hourly and weight daily
Administer antiemetics for food and fluid retention
111.
INTRACELLULAR FLUID VOLUMEDEFICIT
111
Severe hypernatremia and dehydration can cause
ICFVD.
Relatively rare in healthy adults.
common in elderly people and in those conditions
that result in acute water loss.
Symptoms include confusion, coma, and cerebral
hemorrhage.
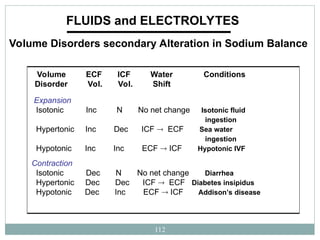
112.
112
FLUIDS and ELECTROLYTES
VolumeDisorders secondary Alteration in Sodium Balance
Expansion
Isotonic Inc N No net change Isotonic fluid
ingestion
Hypertonic Inc Dec ICF ECF Sea water
ingestion
Hypotonic Inc Inc ECF ICF Hypotonic IVF
Contraction
Isotonic Dec N No net change Diarrhea
Hypertonic Dec Dec ICF ECF Diabetes insipidus
Hypotonic Dec Inc ECF ICF Addison’s disease
Volume ECF ICF Water Conditions
Disorder Vol. Vol. Shift


![Clinical calculation of PLASMA OSMOLALITY:
21
PLASMA OSMOLALITY (mOsm/kg of water) =
2(Na+
) + [glucose (mg/dl )/18] + [urea mg/dl /2.8]
Roughly: 2(plasma Na+
) = 2 x 145 mEq/L = 290 mOsm/kg of H2O
Na+ biggest determinant of serum osmolality](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-21-320.jpg)
![49
Patients of Congestive Heart Failure /
Hypertension
treated with angiotensin-converting enzyme (ACE)
inhibitors (e.g., captopril) to lower ECFV & BP
Inhibition of ACE lowers the convesrion of
angiotensin I to II
lowers plasma [angiotensin II]](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-49-320.jpg)
![60
Hypernatremia - Management
Lower serum Na+
Administration of hypotonic sodium solution [0.3 or 0.45%]
Rapid lowering of sodium can cause cerebral edema
Slow administration of IV fluids with the goal of reducing sodium not
more than 08 to 10 mEq/L for the first 48 hrs decreases this risk
In case of Diabetes insipidus desmopressin acetate nasal spray is used
Dietary restriction of sodium in high risk clients
60](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-60-320.jpg)
![Hyponatremia - management
64
Identify the cause and treat
Administration of sodium orally, by NG tube or
parenterally
For patients who are able to eat & drink, sodium is easily
accomplished through normal diet
For those unable to eat, Ringer’s lactate solution or isotonic
saline [0.9%Nacl]is given
For very low sodium 3%Nacl may be indicated
water restriction in case of hypervolaemia](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-64-320.jpg)
![Hyperkalemia - Lab findings
67
serum potassium of 5.3mEq/L results in peaked T
wave HR 60 to 110
serum potassium of 7mEq/L results in low broad P-
wave
serum potassium levels of 8mEq/L results in no
arterial activity[no p-wave]](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-67-320.jpg)
![70
Hyperkalemia- management
Dietary restriction of potassium for potassium
Mild hyperkalemia can be corrected by improving output
by forcing fluids, giving IV saline or potassium wasting
diuretics
Severe hyperkalemia is managed by
1.infusion of calcium gluconate to decrease the antagonistic effect
of potassium excess on myocardium
2.infusion of insulin and glucose or sodium bicarbonate to
promote potassium uptake
3.sodium polystyrene sulfonate [Kayexalate] given orally or
rectally as retention enema](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-70-320.jpg)
![Hypokalemia - Management
76
Mild hypokalemia[3.3to 3.5] can be managed by
oral potassium replacement
Moderate hypokalemia
K-3.0to 3.4mEq/L need 100to 200mEq/L of IV
potassium for the level to rise to 1mEq/L
Severe hypokalemia K- less than 3.0mEq/L
need 200to 400 mEq/L for the level to rise to l
mEq/L
Dietary replacement of potassium helps in
correcting the problem[1875 to 5625 mg/day]](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-76-320.jpg)
![ETIOLOGY AND RISK FACTORS
90
Severe vomiting.
Diaphoresis.
Traumatic injuries.
Third space fluid shifts
[percardial, pleural,
peritoneal and joint
cavities]
Fever.
Gastrointestinal suction.
Ileostomy.
Fistulas.
Burns.
Hyperventilation.
Decreased ADH
secretions.
Diabetes insipidus.
Addison’s disease or
adrenal crisis.
Diuretic phase of acute
renal failure.
Use of diuretics.](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-90-320.jpg)

![Management of Hyperosmolar fluid volume
deficit
95
Administration of hypotonic IV solution , such as 5%
dextrose in 0.2 %saline
If the deficit has existed for more than 24
hours,avoid rapid correction of fluid [sodium
solution to be infused at the rate of 0.5 to 0.1m Eq/
L/ hr]](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-95-320.jpg)
![LAB INVESTIGATION
100
serum osmolality <275mOsm/ kg
Low , normal or high sodium
Decreased hematocrit [ < 45%]
Specific gravity below 1.010
Decreased BUN [< 8mg/ dl]](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-100-320.jpg)
![MANAGEMENT
101
Diuretics [combination of potassium sparing and
potassium depleting diuretics]
In people with CHF, ACE inhibitors and low dose of
beta blockers are used
A low sodium diet](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-101-320.jpg)
![ETIOLOGY
107
Administration of excessive amount of hyposmolar
IV fluids[0.45%saline or 5%dextrose in water]
Consumption of excessive amount of tap water
without adequate nutritional intake
SIADH
Schizophrenia[compulsive water consumption]](https://image.slidesharecdn.com/5-260202070054-ea2e3d42/85/5-Fluid-and-electrolytes-imbalance-2-ppt-107-320.jpg)