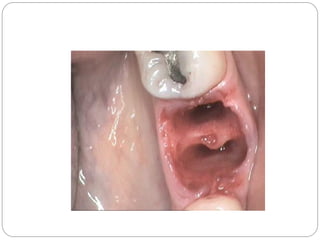
Dry socket, or alveolar osteitis, is a delayed healing of the extraction socket without infection. It occurs when the blood clot fails to form or is dislodged from the socket, exposing bare bone. Common causes include poor blood flow, infection, trauma, or improper rinsing after extraction. A 45-year-old diabetic man presented with severe pain in his lower left jaw 3 days after a tooth extraction. Examination revealed an empty socket with exposed bone and food debris. Radiographs did not show any abnormalities. He was diagnosed with dry socket based on the clinical presentation. The socket was irrigated and dressed with a medicated dressing to manage pain until it subsided in a few days with


![Dry socket[1], alveolar ostitis (2),](https://cdn.slidesharecdn.com/ss_thumbnails/drysocket1-160126190015-thumbnail.jpg?width=640&height=640&fit=bounds)












































