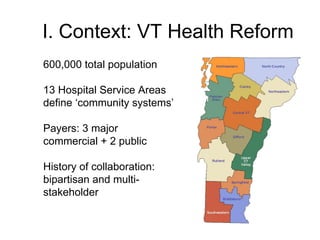
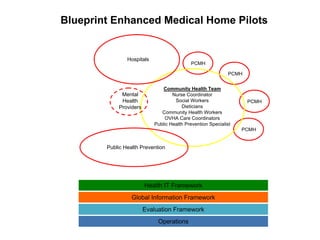
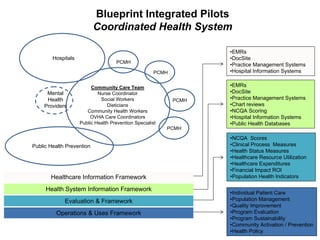
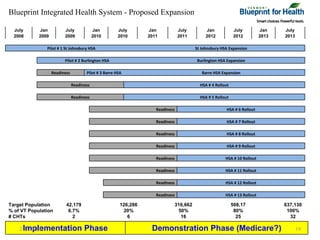
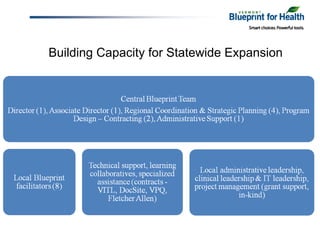
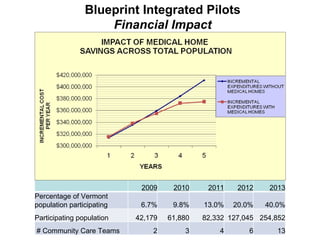
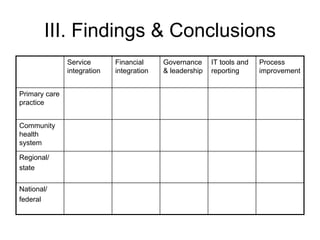
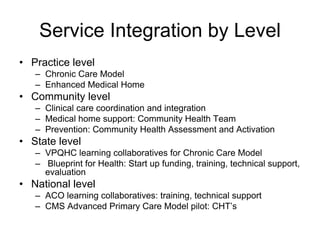
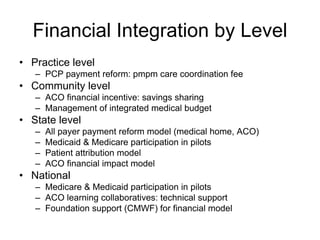
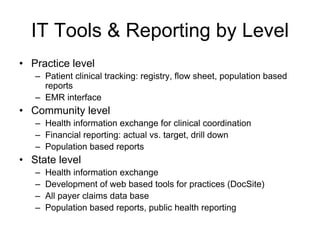
The document summarizes a webinar discussing Vermont's development of a pilot community health system to achieve the "triple aims" of improved health, improved care, and reduced costs. It outlines Vermont's health reform context and strategy, including efforts to reduce the uninsured rate, expand health IT, and reform delivery systems. It then describes pilots to enhance medical homes at the practice level, develop accountable care organizations (ACOs) at the community level, and integrate services, financing, governance, information, and process improvement across multiple levels of the system. The goal is to determine if this community health system approach can strengthen primary care, increase preventive care and chronic disease management, and shift costs from episodic to preventive care.