Downloaded 27 times


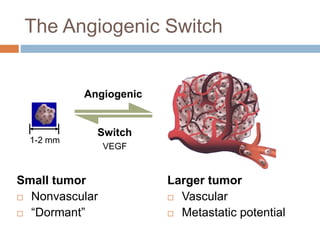
![Risk Factors for Lung Cancer
Smoking
Lung cancer deaths due to smoking
~ 91% males and 80% females[1]
Environmental factors[2]
Second-hand smoke 3% to 5%
Radon 3% to 5%
Industrial pollution 0% to 5%
Radiation exposureRare
Asbestos, radon, radiation, silicosis, and berylliosis
Arsenic exposure, talc, obesity, genetic factors
1. CDC. Lung Cancer. 2011.
2. American Cancer Society. Lung Cancer. 2011.](https://image.slidesharecdn.com/2003ppt-140710064545-phpapp02/85/2003-ppt-5-320.jpg)
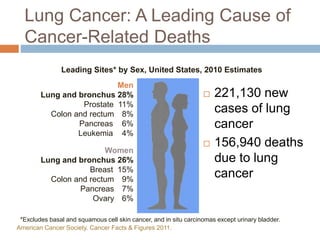
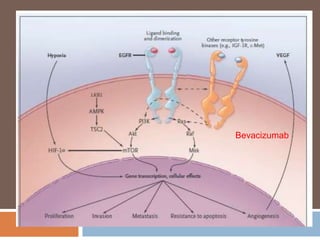
![Lung Cancer Subtypes
The WHO classification for primary lung cancer recognizes 4 major
histology types[1]
Small-cell
carcinoma
13.0%
Large-cell
carcinoma
5.0%
Adenocarcinoma
38.3%
19.7%
Squamous cell
carcinoma
Other*
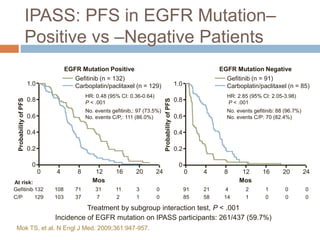
24.0%
Percent distribution by histology among histologically
confirmed lung cancer cases, 2001-2004[2]
1. Brambilla E, et al. Eur Respir J. 2001;18:1059-1068.2. SEER Database. Lung and Bronchus Cancer
(Invasive), 1975-2004.
*Including adenosquamous
carcinoma; carcinomas with
pleomorphic, sarcomatoid or
sarcomatous elements;
carcinoid tumor; carcinomas of
salivary gland type; and
unclassified carcinoma](https://image.slidesharecdn.com/2003ppt-140710064545-phpapp02/85/2003-ppt-7-320.jpg)
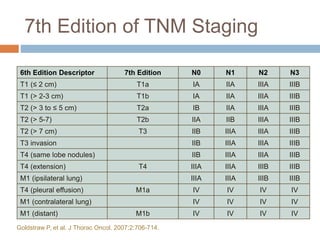
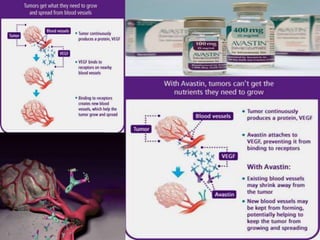
![Chemotherapy vs Best Supportive
Care in Advanced NSCLC: Meta-
Analysis
Meta-analysis of 8 trials (778 patients) using
cisplatin-based chemotherapy[1]
Absolute improvement in survival of 10% at 1 yr[1]
Median survival, BSC vs chemo: 4 vs 8+ mos,
respectively
Median survival now 12+ mos in more recent
trials
VEGF-targeted therapy plus platinum doublet[2]
Quality-of-life benefit from chemotherapy[3]
1. NSCLC Collaborative Group, et al. BMJ. 1995;311:899-909. 2. Herbst R, et al. Clin Lung Cancer.
2009;10:20-27 3. Klastersky J, et al. Lung Cancer. 2001;34(suppl 4):S95-S101.](https://image.slidesharecdn.com/2003ppt-140710064545-phpapp02/85/2003-ppt-9-320.jpg)
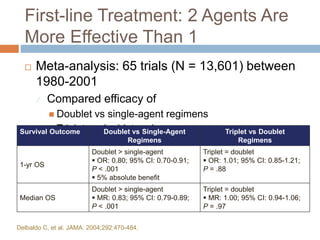
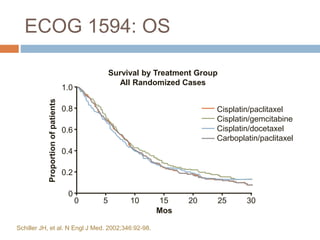
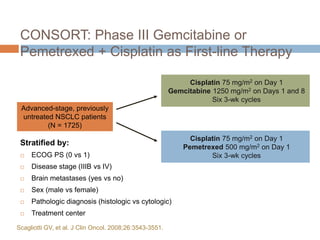
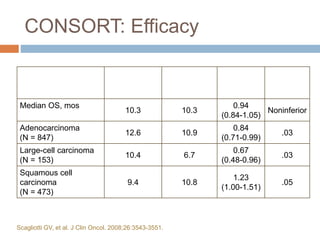



This document discusses therapeutic options for first line treatment of advanced non-small cell lung cancer (NSCLC). It provides details on chemotherapy regimens such as platinum doublets with paclitaxel, gemcitabine or docetaxel. It also discusses targeted therapies like bevacizumab, erlotinib and gefitinib. The document reviews clinical trials that established current standard first line treatments and highlights the need for personalized treatment based on tumor markers and mutations.
















































































