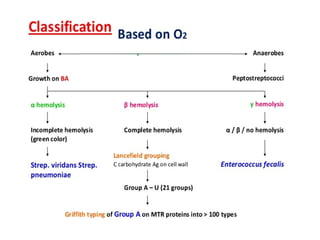
Classification contd
• βhemolytic Streptococci is further divided into Lancefield groups A-V
depending on the group specific carbohydrate
• Without I and J
• Group A is S.pyogenes which is further classified depending on the
MTR protein in the cell wall of bacteria known as Griffith typing
about 80 serotypes are present.
8.
Toxins and Enzymesproduced
• Haemolysins 2 types
• Streptolysin O – oxygen labile heat labile strongly antigenic
contributes to virulence
• Streptolysin S – oxygen stable non antigenic and nephrotoxic
• Erythrogenic toxin- heat stable cause erythema, responsible
for scarlet fever and streptococcal toxic shock syndrome
9.
•Streptokinase- heat stable,antigenic, lysis of human
fibrin clots. Hence play an important role in
breaking down of the fibrin barrier around the
lesion and cause spreading infection.
•Deoxyribonuclease – depolymerisation of DNA,
liquifies pus.
•Diphosphopyridine nucleotidase- leucotoxic
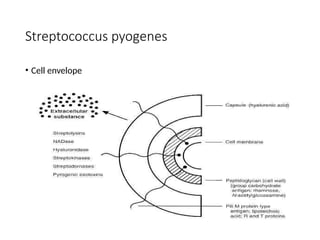
Pathogenicity of Spyogenes
• Much more dangerous organism
• Can cause septicaemia
• Carrier rate is 5 % in man
• Carriers and patients are the sources of infection
• Transmission - Droplets, direct or indirect contact
Cause
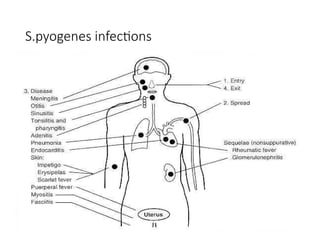
1. Suppurative diseases
2. Non suppurative diseases
13.
Pathogenicity of S.pyogenes
suppurativediseases
• The main site of streptococcal infection is throat, sore
throat. In children infection is more diffuse leading to
pharyngitis than tonsillitis.
• From throat it can spread to different sites causing
otitis media, Mastoiditis, meningitis,Ludwigs angina,
pneumonia and suppurative adenitis
• Skin infection- wounds and burns infection causing
lymphangitis and cellulitis a complication that may
lead to septicaemia
14.
Skin infection
• Erysipelas– involving the superficial layer of skin.It becomes
swollen red and indurated.
• Impetigo seen in children this may lead to glomerulonephritis
16.
•Genital infection- puerpuralsepsis
•Females use to die of this infection due to aseptic
techniques used during delivery
•Other suppurative lesions include abscess in the
lung,liver,kidney, brain which may lead to
septicaemia and pyaemia.
17.
Non suppurative complications(post
Streptococcal sequelae)
• Usually seen after 3 weeks of initial infection and
organism is no longer detected in this stage,
antibodies to extracellular antigens can be seen.
• Acute rheumatic fever
• Connective tissue degeneration of the cardiac
valves
• Carditis
18.
•Infective myocardial lesionswith Aschoff’s
nodules due to the hypersensitivity to
structural component antigenic cross
reaction between structural antigen of
S.pyogenes and cardiac tissues. Any serotype
of S.pyogenes can cause infection.
(1,3,5,6,12,14)
19.
Case History
• A10 year old boy
• Presented Skin infection
• Five days later, coloured urine and pitting oedema
• Elevated BP, 4+ proteinuria, elevated serum creatinine
• Whats the Diagnosis?
• What are the investigation required?
20.
•Acute glomerulonephritis
•Only nephritogenicstrains cause this infection
•Usually after skin infection
•Causes nephritis which is self limited without any
permanent damage, due to cross reaction between
glomerular antigen and antigenic component of
nephritogenic strain, immune complex disease
21.
Differences between ARFand AGN
• Acute rheumatic fever
• Site of infection is throat
• Serotype- any
• Immune response-
marked
• Acute glomerulonephritis
• Skin or throat
• Nephritogenic strains
12,2,4,52,55,57
• Immune response is
moderate
Laboratory diagnosis
• Specimens(pikes medium can be used)
• Morphology- Grams staining
• Direct fluorescence antibody test
• Culture- aerobic and facultative anaerobe,
fastidious, blood,serum,glucose favours the growth
of the organism
25.
Laboratory diagnosis
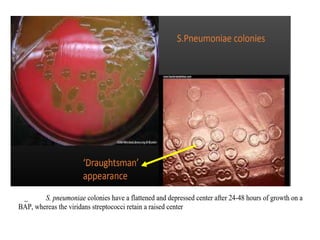
Blood agar:pinpoint, circular, transparent, low convex colonies with clear
area of beta hemolysis, virulent strains produce granular colonies
•Fluid media: Granular turbidity with powdery deposit in 24 hrs.
•Selective media- Crystal violet blood agar
26.
Biochemical reactions
• Fermentsglucose,lactose, salicin and sorbitol with acid only.
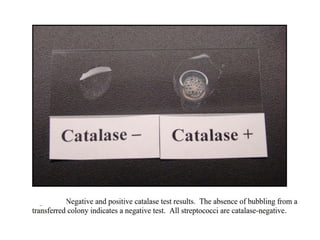
• Catalase test is negative.
• Liquefies gelatin.
• Insoluble in 10% bile.
Serological test
• AntistreptolysinO (ASO test)
• >200 units
• Antideoxyribonuclease B (ADNaseB)
• >300-350 units
• AntiHyaluronidase test
• Streptozyme test
Group B streptococci
•S.agalactiae
• Neonatal meningitis and septicaemia especially after delivery
• Osteomyelitis, arthritis, conjunctivitis, endocarditis & respiratory
infections
• Septic abortion and puerpural sepsis in females
31.
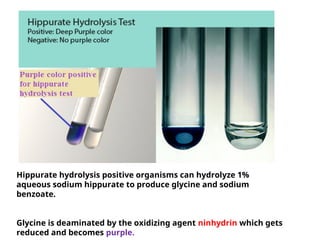
Hippurate hydrolysis positiveorganisms can hydrolyze 1%
aqueous sodium hippurate to produce glycine and sodium
benzoate.
Glycine is deaminated by the oxidizing agent ninhydrin which gets
reduced and becomes purple.
32.
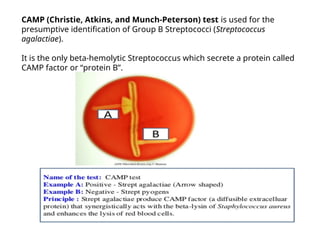
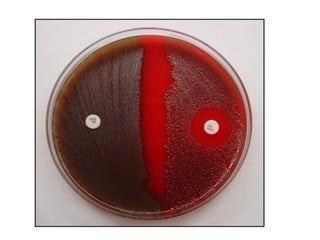
CAMP (Christie, Atkins,and Munch-Peterson) test is used for the
presumptive identification of Group B Streptococci (Streptococcus
agalactiae).
It is the only beta-hemolytic Streptococcus which secrete a protein called
CAMP factor or “protein B”.
Clinical significance:
•Enterococcus faecalisis a Gram-positive, commensal bacterium inhabiting the
gastrointestinal tracts of humans and other mammals.
•E. faecalis can cause life-threatening infections in humans, especially in the
nosocomial (hospital) environment.
Eg.
•Urinary tract infections (UTI)
•Bacteremia
•Endocarditis
•Meningitis
•E. faecalis is resistant to many commonly used antimicrobial agents.
•VRE (Vancomycin-Resistant Enterococcus)
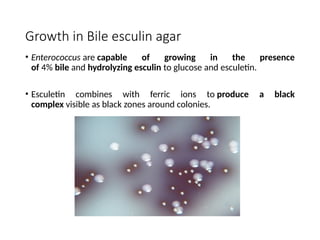
Growth in Bileesculin agar
• Enterococcus are capable of growing in the presence
of 4% bile and hydrolyzing esculin to glucose and esculetin.
• Esculetin combines with ferric ions to produce a black
complex visible as black zones around colonies.
37.
Case History
• A68 year old man who developed a harsh, productive cough four days
prior to being seen by a physician.
• The sputum is thick and yellow with streaks of blood.
• He developed a fever, shaking, chills and malaise along with the cough.
• O/E: blood pressure 152/90, heart rate 112/minute and regular,
respiratory rate 24/minute and somewhat labored, temperature 103.6.
• On auscultation: late inspiratory crackles are heard in the area of the
right mid-anterior and right mid-lateral lung fields.
• Investigation: WBC 17,000/mm3; neutrophils 70%, lymphocytes 15%.
• Following a chest x-ray PA view and Lateral which revealed an acute
pneumonia in the right middle lobe.
38.
• Sputum wassend to lab for culture and sensitivity
• On gram stain: Gram positive capsulated cocci are seen in pairs
• Diagnosis??
• The patient was treated with antibiotics as an outpatient. During the
10 days of treatment the patient's fever abated and he felt somewhat
better
ANTIGENIC PROPERTIES
•CAPSULE :The most important antigen of
S.pneumonia is the type specific capsular
polysaccharide.
•As this polysaccharide diffuses into the culture
medium or infective exudates and tissues , it is also
called “specific soluble substance” (SSS)
• S.pneumonia are classified based on antigenic
nature of capsular polysaccharide .
•More than 90 serotypes are recognized named 1,2,3
.. etc
43.
Transmission
• Most infectionsare caused by endogenous spread from the
colonized nasopharynx or oropharynx to distal site (e.g.,
lungs, sinuses, ears, blood, meninges)
• Person-to-person spread through infectious droplets
• Typically a secondary infection (after the flu, etc.)
• Young children and the elderly are at greatest risk for
meningitis
45.
Case history
• A32-year-old male was admitted with a 4-day history of left otalgia,
headache and fever (38 °C).
• Otoscopic examination showed purulent otorrhea in the left external
meatus and the left tympanic membrane was slightly hyperaemic,
but no swelling or tenderness were noted in the external auditory
meatus or in the retroauricular area.
• Patient had history of chronic sinusitis
• S.pnemoniae was isolated from ear swab and sinuses drain
• After 24 hours, the patient developed photophobia, vomiting and
neck rigidity. Blood cell count showed leukocytosis (25,000) and
neutrophilia (93.0%).
• Cerebro-spinal fluid (CSF) analysis disclosed increased levels of total
proteins (178 mg/dl), leukocytosis (220/mm3
) and normal pressure
• Diagnosis???
48.
Laboratory diagnosis
Specimen:
•Sputum
•CSF
•blood forculture
•urine are used for antigen detection
Microscopy: Gram-stained smear of samples contain gram-positive
diplococci both inside polymorphs and extracellularly.
49.
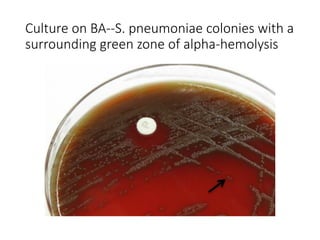
Culture on BA--S.pneumoniae colonies with a
surrounding green zone of alpha-hemolysis
53.
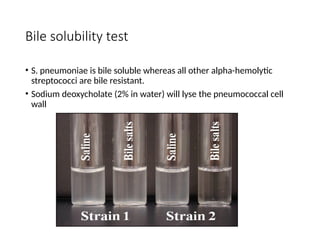
Bile solubility test
•S. pneumoniae is bile soluble whereas all other alpha-hemolytic
streptococci are bile resistant.
• Sodium deoxycholate (2% in water) will lyse the pneumococcal cell
wall
54.
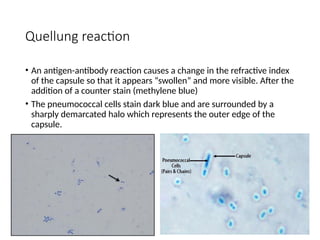
Quellung reaction
• Anantigen-antibody reaction causes a change in the refractive index
of the capsule so that it appears “swollen” and more visible. After the
addition of a counter stain (methylene blue)
• The pneumococcal cells stain dark blue and are surrounded by a
sharply demarcated halo which represents the outer edge of the
capsule.
56.
Prophylaxis
•Polyvalent polysaccharide vaccinerepresenting the
capsular antigens of 23 most prevalent serotypes
gives 80-90% protection.
•It is meant only for persons who are at increased
risk of pneumococcal infection such as those with
absent or dysfunctional spleen, sickle cell disease,
chronic lung, liver, renal and heart diseases,
diabetes mellitus and immunodeficiencies including
HIV infection.
•It is not recommended under the age of two years
or above 65 years.
57.
•Growth at pHof 9.6
•Heat resistant at 60°C for 30 minutes
•Mac Conkey’s agar: pinpoint deep pink colored
colonies are produced.
58.
Enterococcus infections
• UTI
•Wound infections
• Biliary tract Infections
• Intra abdominal abscess
• Antibiotic sensitivity should be performed as drug resistance is common
in this bacteria
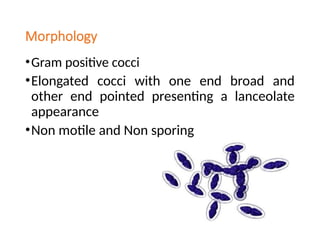
Morphology
Gram positiveBacilli
Largest pathogenic bacteria
Spores are produced in the soil and
culture not in animal tissue
Capsulated made up of polypeptide
62.
Pathogenicity
Zoonotic disease
Primarily a disease of cattle and
sheep
Main virulence is due to the exotoxin
complex
3 fractions- Protective antigen,
oedema factor and lethal factor
Capsule which prevents phagocytosis
63.
Human anthrax -3types
Cutaneous anthrax the most
common type of anthrax
Lesions starts with papules, vesicles
The whole area becomes congested
oedematous and several satellite like
lesions are formed- black eschar
Malignant pustule
65.
Pulmonary anthrax-due to inhalation
of the dust of the infected wool.
Wool sorter’s disease
66.
Intestinal anthrax
Mainly seen in primitive communities
Who used to eat caracasses of the
animals died of Anthrax
Violent enteritis and bloody diarrhoea
67.
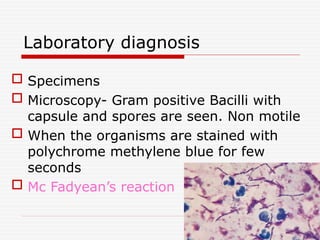
Laboratory diagnosis
Specimens
Microscopy- Gram positive Bacilli with
capsule and spores are seen. Non motile
When the organisms are stained with
polychrome methylene blue for few
seconds
Mc Fadyean’s reaction
68.
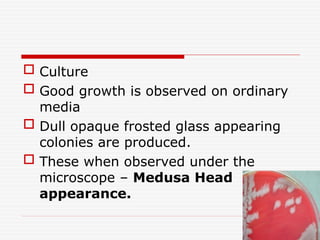
Culture
Goodgrowth is observed on ordinary
media
Dull opaque frosted glass appearing
colonies are produced.
These when observed under the
microscope – Medusa Head
appearance.
69.
The bacilliare arranged end to end
giving a Bamboo stick appearance.
Colonies are non haemolytic on blood
agar.
Selective medium is PLET MEDIUM.
70.
Biochemical reactions
Catalasetest is positive
Glucose maltose sucrose fermented
with the production of acid only.
Gelatin is liquified
Nitrate is reduced to nitrite.
71.
Serology –Ascoli’s thermoprecipitation
test and Complement Fixation Test.
Animal pathogenicity
Guinea pigs injected subcutaneously with
suspension of bacilli.
Animal dies in 24-72 hours
Bacteria are found in large numbers in
the local lesions, heart blood and spleen.
72.
PROPHYLAXIS
Proper sterilisationof Animal products
like hide and wool.
Animals and high risk group
individuals should be immunised
Treatment – penicillin, streptomycin,
ciprofloxacin.
In themeninges it causes the suppurative lesions of
the spinal cord and the brain.
Sequalae in survivors is blindness, deafness and
chronic meningitis
Bacteraemia can cause chills malaise and
prostrations petechial lesions in the skin and the
mucosa
Toxin released can cause haemmorhage and
profound shock – WATERHOUSE FRIDERICHSEN
SYNDROME.
78.
laboratorydiagnosis
Specimen collection
CSF divided into 3 parts
One part used for
Grams staining
Second part is used for culture
Another part is incubated and cultured after
24 hours.
79.
Blood culture
Nasopharyngeal swabs to detect carriers
Petechial lesions specimens can be cultured
80.
culture
Strict aerobe
Blood agar- small transluscent smooth grey colonies
are produced
Chocolate agar
Selective medium – Modified Thayer Martin
medium
Biochemical reactions- catalase and oxidase test
positive, glucose and maltose is fermented with
production of acid only.
Pathogenicity
STD
Gonorrhoea
There is adhesion of gonococci to urethral
mucosal surface
Cocci penetrates intracellular spaces and
subepithelial connective tissue
84.
In males
Inflammationof the urethra, prostate, seminal
vesicles, epididymis
Stricture of the urethra, periurethral tissue
infection, abscess and multiple discharging
sinuses ‘ water can perineum’
85.
In females
Inprepubertal girls – vulvovaginitis, they act
as carriers of the organism and the infections
spreads to fallopian tubes and endometrium.
86.
In both thesexes
Proctitis
Conjunctivitis
Metastatic lesions – arthritis, endocarditis,
meningitis pyaemia.
Ophthalmia neonatorum
87.
Laboratory diagnosis
Specimencollection
Urethral discharge, cervical swabs
Grams staining
Culture
Chocolate agar – small around transluscent
convex colonies are produced.
Selective medium – modified thayer martin
medium
88.
Lab diagnosis
Biochemicaltests : catalase and oxidase test is
positive.
Glucose is fermented but not Maltose.
Serology – Chronic and metastatic lesions
Precipitation, agglutination,
Immunofluorescence test and RIA.