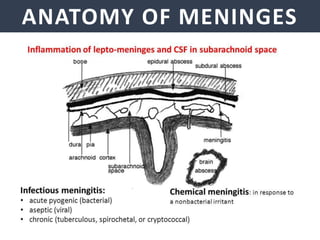
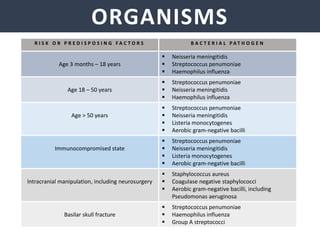
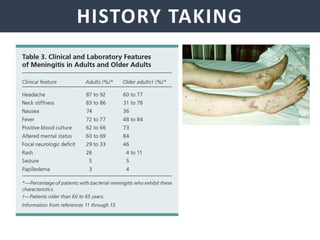
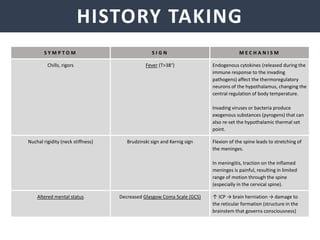
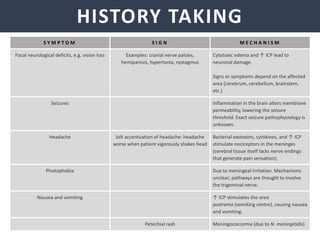
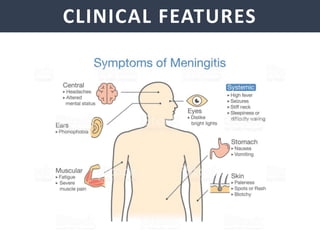
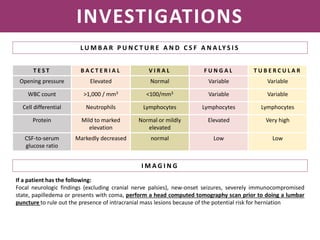
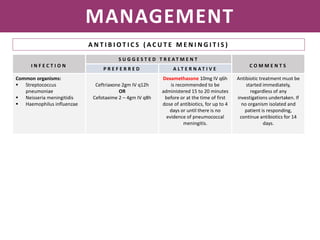
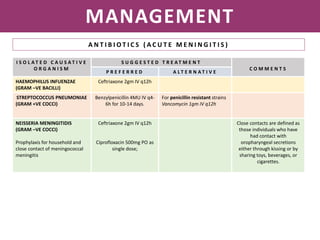
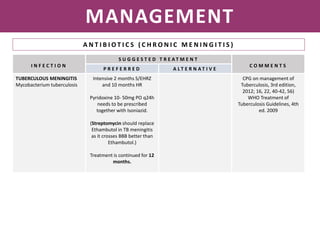
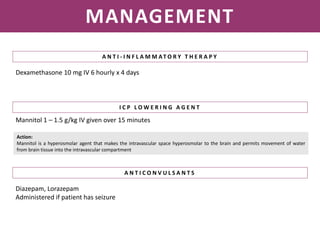
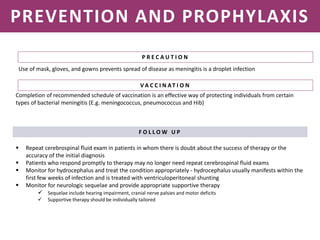
Meningitis is an inflammation of the meninges that covers the brain and spinal cord. It can be caused by bacterial, viral, or fungal infections. The main symptoms include headache, fever, stiff neck, nausea, confusion, and seizures. A physical exam may reveal neck stiffness, rashes, and cranial nerve abnormalities. Prompt diagnosis and treatment are important as meningitis can progress rapidly and cause permanent damage or death if not treated. The most common causes are Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae.