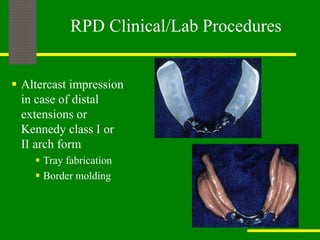
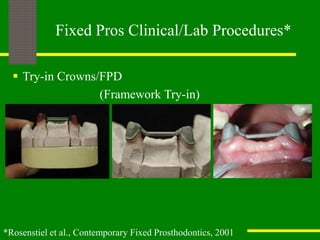
This document outlines a treatment planning protocol for complex prosthodontic cases in dental school clinics. It describes developing diagnostic models and wax-ups to evaluate treatment options. The protocol involves multiple phases including diagnosis, disease control, restorative treatment, and maintenance. Clinical procedures are outlined for removable partial dentures, fixed prosthetics, and immediate dentures. Following this protocol helps provide higher quality care, enhance student learning, and improve efficiency.