This document discusses health education and its importance. It defines health education as informing, motivating, and helping people adopt and maintain healthy practices. The key points are:
- Health education aims to ensure communities value health, equip people with skills to solve health problems themselves, and promote proper use of health services.
- Models of health education include cognitive (providing information), motivational (addressing barriers to applying information), and social intervention (addressing prerequisites for health like income, food, shelter).
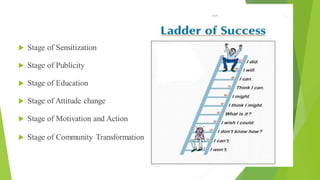
- The principles of effective health education are interest, participation, starting from known concepts, comprehension, reinforcement, motivation, learning by doing, using respected leaders, and building good relationships.
- The process





















![Unit 8 Health education (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/unit8healtheducation1autosaved-241027173916-a26c0100-thumbnail.jpg?width=640&height=640&fit=bounds)