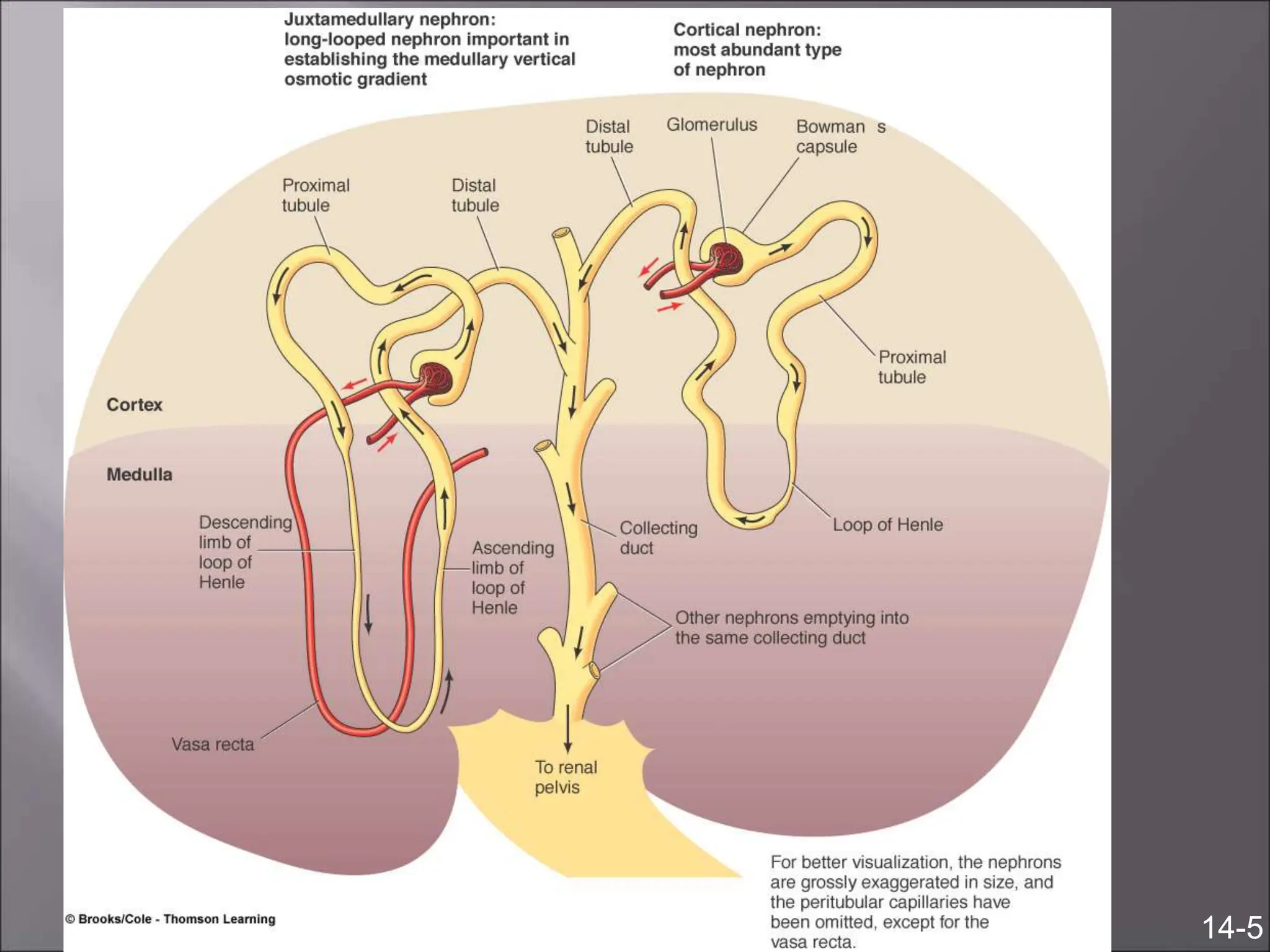
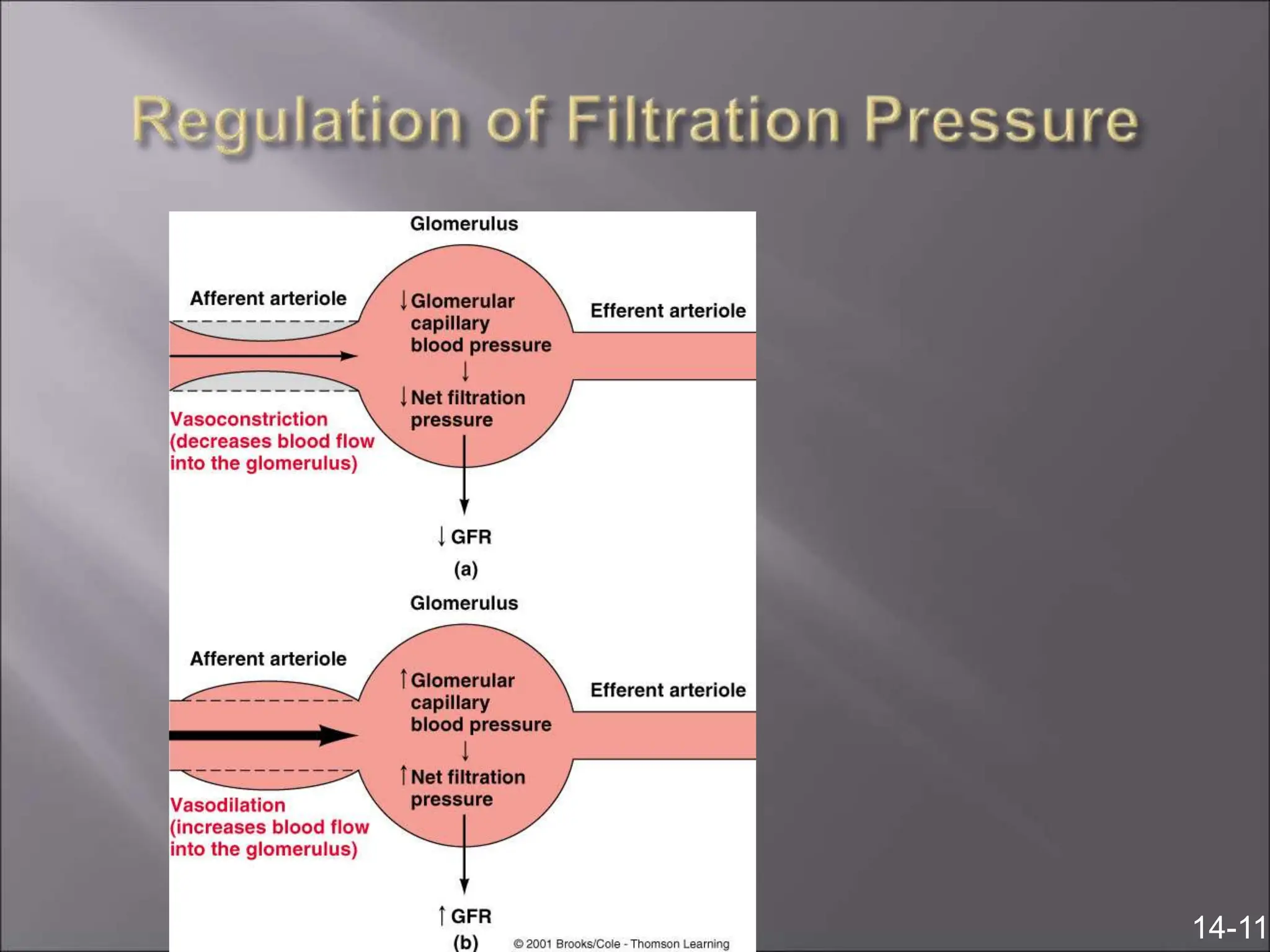
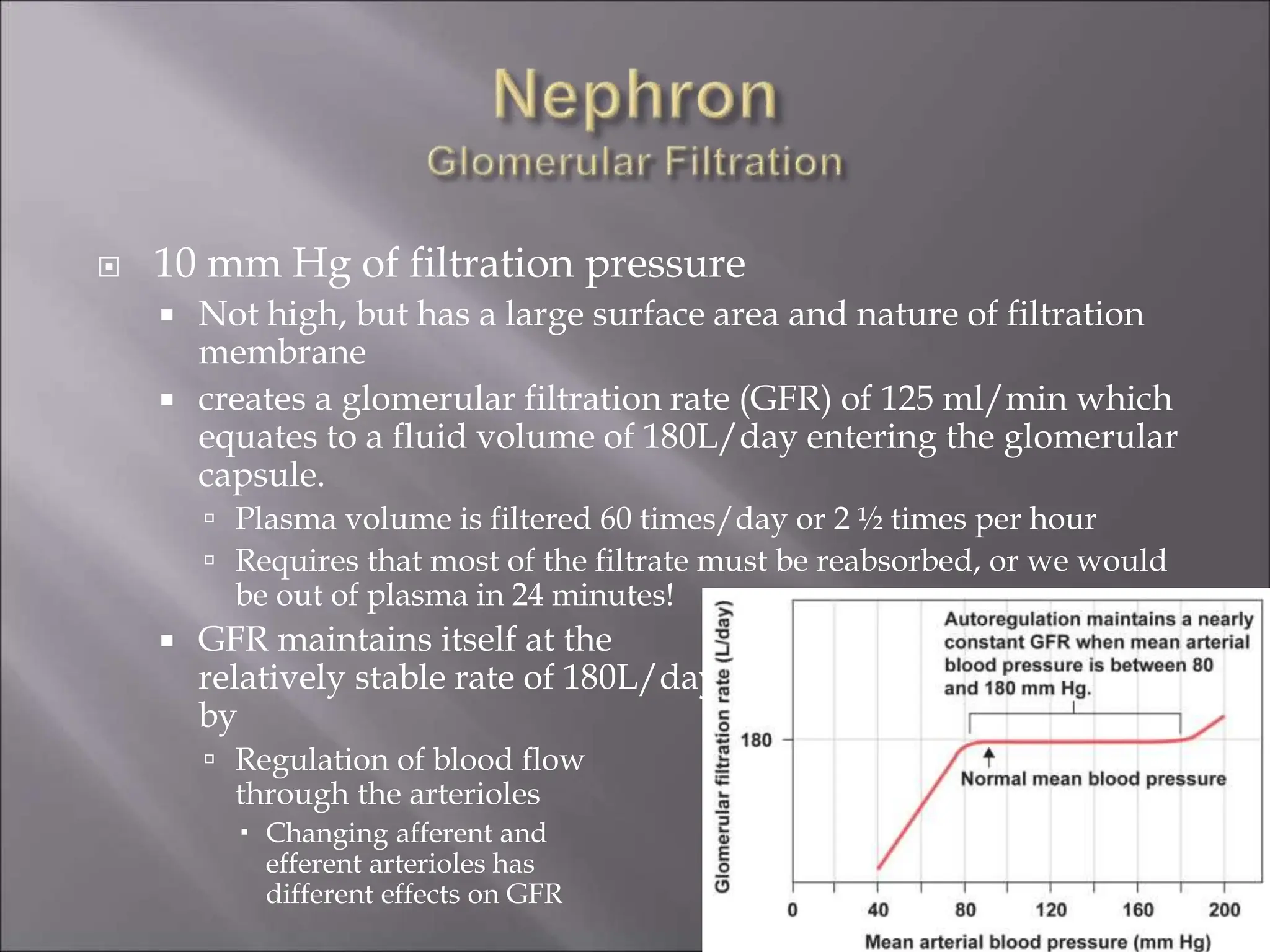
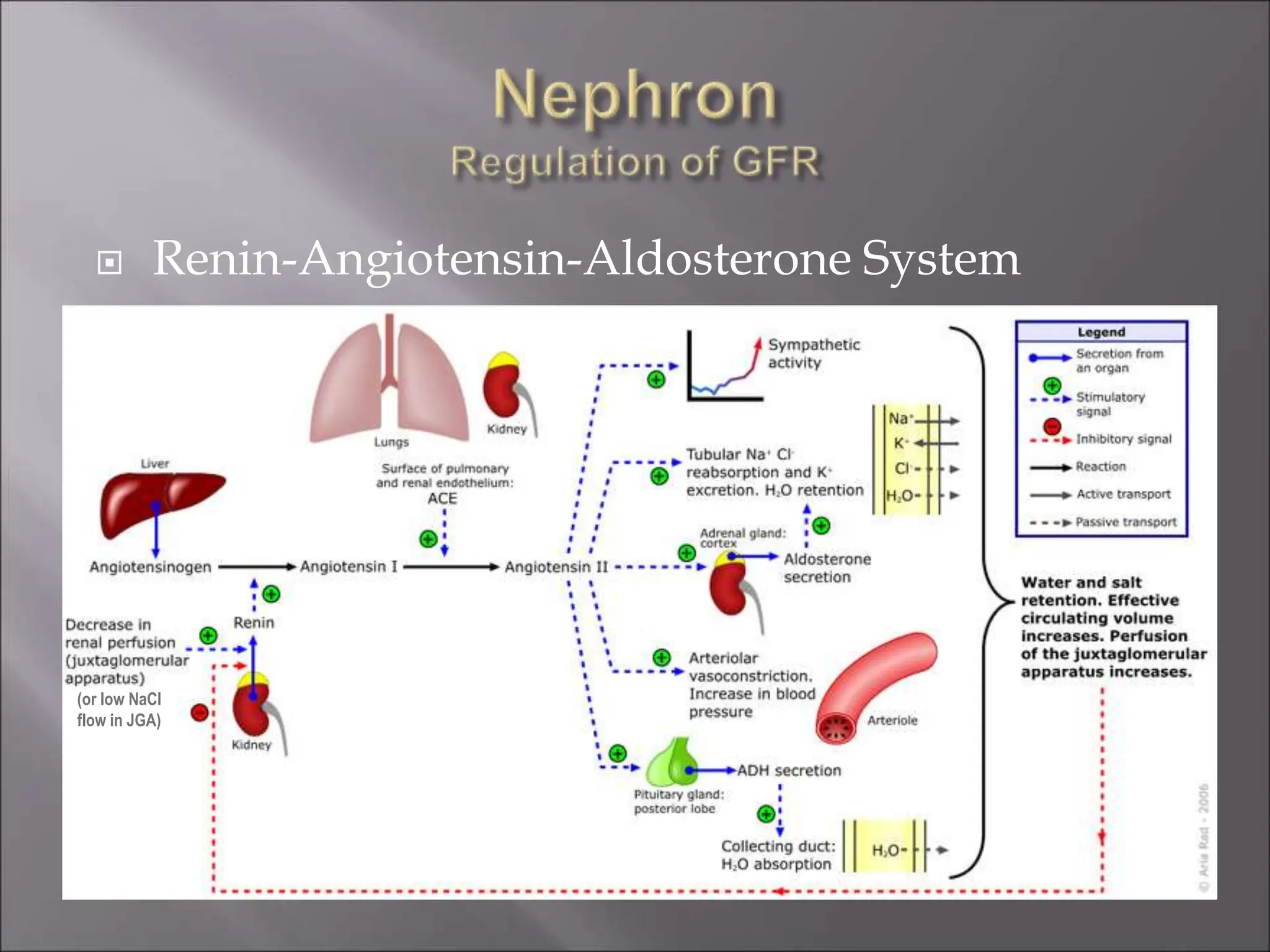
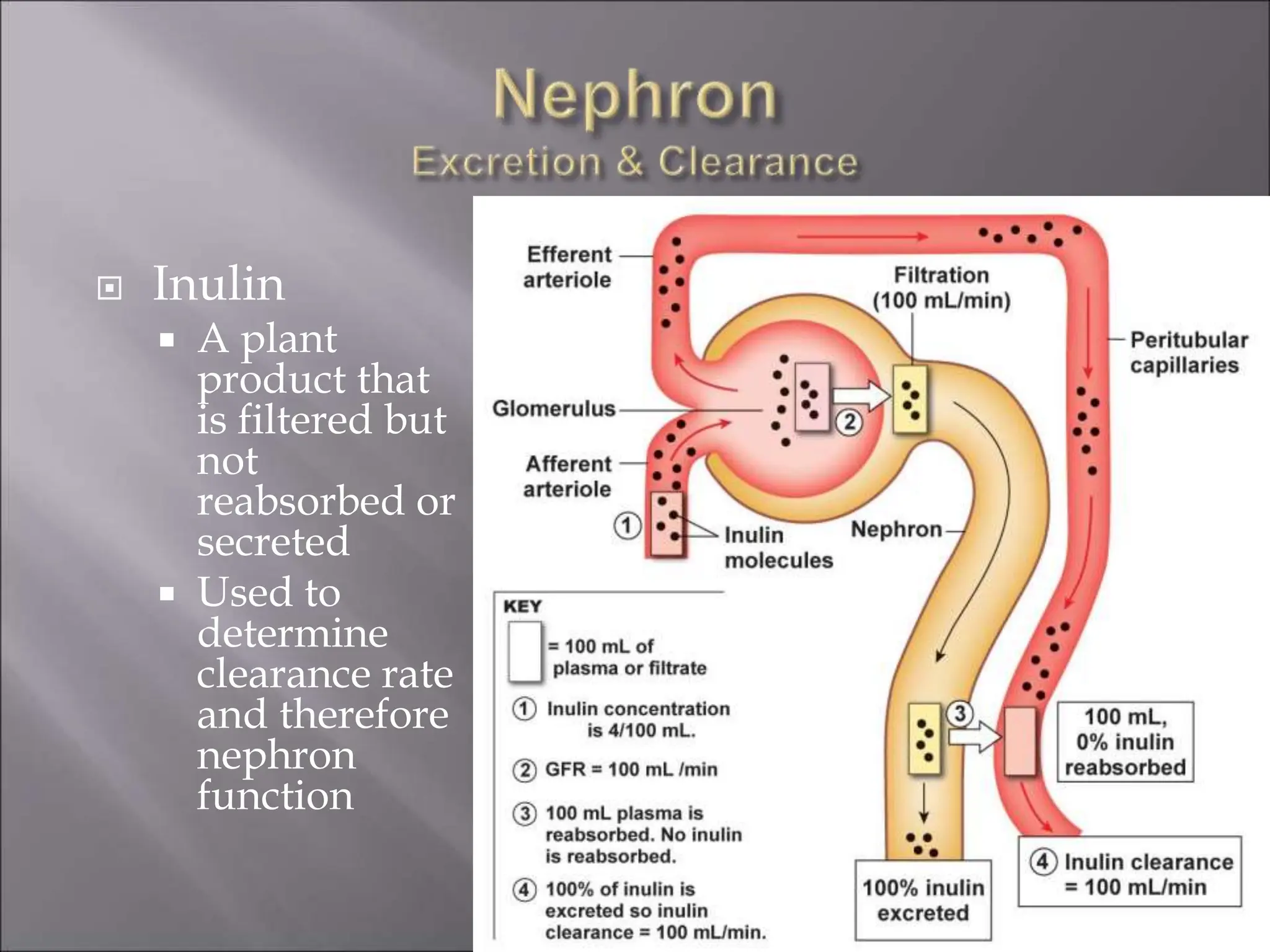
The nephron is the functional unit of the kidney that filters blood to produce urine. It consists of a glomerulus for blood filtration and a tubule for reabsorption and secretion. The kidneys regulate fluid volume and composition by precisely controlling glomerular filtration, tubular reabsorption and secretion. Hormones and the renin-angiotensin system help maintain stable glomerular filtration rate despite changes in blood pressure.
















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









