Model Call Girl in Tilak Nagar Delhi reach out to us at 🔝9953056974🔝
Poster chest masses
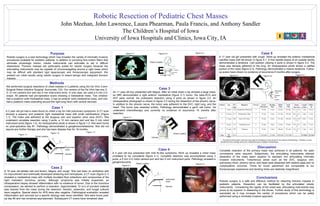
1. Robotic Resection of Pediatric Chest Masses John Meehan, John Lawrence, Laura Phearman, Paula Francis, and Anthony Sandler The Children’s Hospital of Iowa University of Iowa Hospitals and Clinics, Iowa City, IA Purpose Robotic surgery is a new technology which may broaden the variety of minimally invasive procedures available for pediatric patients. In addition to providing fine-motion filters that eliminate physiologic tremor, robotic instruments can articulate to aid in difficult dissections. Thoracic masses are particularly suited for robotic surgery because the articulating instruments may be capable of circumnavigating around a rigid mass which may be difficult with standard rigid laparoscopic and thoracoscopic equipment. We present our initial results using robotic surgery to resect benign and malignant thoracic masses. Methods We performed surgical resections of chest masses in 5 patients using the Da Vinci 3-arm Surgical Robot (Intuitive Surgical, Sunnyvale, CA). Our version of the Da Vinci has one 3-D 12 mm camera arm and two 5 mm instrument arms. In one case, we used a 5 mm 2-D scope. All patients had pre-operative scans showing a mediastinal mass. Two children had a posterior solid mediastinal mass, 2 had an anterior solid mediastinal mass, and one had a posterior mass extending around the right lung hilum with central necrosis. Case 1 A 2 year old girl had a mass found on chest x-ray for mild pulmonary symptoms. A CT scan showed a superior and posterior right mediastinal mass with small calcifications (Figure 1-1). The mass was adherent to the azygous vein and superior vena cava (SVC). She underwent complete resection using 3 ports; a 12 mm camera port and two 5 mm robot instrument ports (figure 1-2). An intraoperative photo is shown in figure 1-3. She went home on post-operative day #1. Pathology demonstrated a ganglioneuroblastoma. She did not require any further therapy and she has been disease free for 18 months. Case 3 An 11 year old boy presented with fatigue. After an initial chest x-ray showed a large mass, an MRI demonstrated a right anterior mediastinal (figure 3-1) tumor. His beta-HCG and AFP were normal. He underwent resection using 4 ports as shown in figure 3-2. An intraoperative photograph is shown in figure 3-3 during the dissection of the phrenic nerve. In addition to the phrenic nerve, the tumor was adherent to the SVC, right lung, and the heart. The tumor was resected enbloc. Pathology demonstrated a germ cell tumor. He underwent chemotherapy and currently no evidence of recurrence 15 months after resection. Conclusions Robotic surgery is a safe and effective method for resecting thoracic masses in pediatric patients. Dissection can be facilitated by the articulated robotic instruments. Considering the rigidity of the chest wall, articulating instruments may prove to be superior in dissecting in the thorax. Further study of this technology is warranted as it may increase the variety of procedures which can be safely performed using a minimally invasive approach. Discussion Complete resection of the primary mass was achieved in all patients. No open conversions were required. Subjectively, the articulating instruments allowed dissection of the mass seem superior to standard non articulating minimally invasive instruments. Treacherous areas such as the SVC, azygous vein, pulmonary hilum, phrenic nerve, and heart were dissected with relative ease and no complications occurred. Times for trocar placement are comparable to our thoracoscopic experience and docking times are relatively insignificant. Figure 1-1 Figure 1-3 Figure 1-2 Figure 2-1 Figure 2-3 Figure 2-2 Figure 5-1 Figure 3-2 Figure 3-3 Case 2 A 16 year old athlete had and fevers, fatigue, and cough. She had been on antibiotics with no improvement and eventually developed wheezing and hemoptysis. A CT scan (figure 2-1) revealed a mediastinal mass with multiple loculated fluid collections and compromise of the right mainstem bronchus (arrow). Although lymphoma was initially suspected, an intraoperative biopsy showed inflammation with no evidence of tumor. Due to the bronchus compression, we elected to perform a resection. Approximately 10 cc’s of purulent material was drained from the mass during the resection. Aerobic, anaerobic, and fungal cultures were negative. Special stains for AFB were also negative. Pathological evaluation revealed inflammation and necrosis but a specific etiology was never identified. She went home post-op day #3 and has remained asymptomatic. Subsequent CT scans have remained clear. Figure 3-1 Case 4 A 4 year old boy presented with mild flu-like symptoms. Work up revealed a chest mass unrelated to his complaints (figure 4-1). Complete resection was accomplished using 3 ports; a 5 mm 2-D robot camera port and two 5 mm instrument ports. Pathology revealed a ganglioneuroma. E Robot Location Camera E Robot Location Case 5 A 17 year old girl presented with cough. Work-up revealed the anterior mediastinal calcified mass with fat shown in figure 5-1. A fine needle biopsy at an outside facility demonstrated a teratoma. Cart position utilizing 4 ports is shown in figure 5-2. The mass was densely adherent to the lung. An intraoperative photo shows a calified portion of the mass (figure 5-3). Pathology demonstrated a mature teratoma. Follow-up scans have shown no evidence of recurrence 6 months after surgery. Figure 5-3 Figure 4-3 * - The patient with the germ cell tumor was ready for discharge on post-op day #1 but required chemotherapy. Therefore, he was transferred to the oncology service for 2 additional days of inpatient chemotherapy. Figure 4-1 Accessory Port E Robot Location Camera Instrument Arms Figure 5-2 Phrenic Nerve Robot Location Camera Instrument Arms Robot Location E E Instrument Arms Camera Patient Age Wt. (kg) Diagnosis Trocars Trocar Placement Docking Time Robot Time Total Time Tumor Size (cm) Length of Stay Follow-up 1 2 years 13.9 Ganglioneuroblastoma 3 10 min 3 min 56 min 69 min 6.5 x 4.2 x 1.7 1 day 18 mo. 2 16 years 61.7 Inflammatory Mass 4 10 min 3 min 143 min 156 min 6.0 x 4.0 x 2.0 3 days 15 mo. 3 11 years 40.0 Germ Cell Tumor 4 14 min 4 min 131 min 146 min 12.0 x 14.0 x 5.2 1 day* 15 mo. 4 4 years 21.5 Ganglioneuroma 3 18 min 4 min 22 min 44 min 4.0 x 2.0 x 2.5 1 day 13 mo. 5 17 years 70.5 Teratoma 4 8 min 3 min 140 min 151 min 5.6 x 4.7 x 2.9 1 day 6 mo. Avg. 9.8 years 41.5 - - 12.5 min 3.4 min 98.4 min 113.2 min - 1.4 days 13.4 mo