
Recommended
Recommended
More Related Content
Similar to Exercise 4 Cardiovascular FitnessThis exercise describes thre.docx
Similar to Exercise 4 Cardiovascular FitnessThis exercise describes thre.docx (20)
More from rhetttrevannion
More from rhetttrevannion (20)
Recently uploaded
Recently uploaded (20)
Exercise 4 Cardiovascular FitnessThis exercise describes thre.docx
- 1. Exercise 4: Cardiovascular Fitness This exercise describes three assessments designed to help you estimate the present level of your cardiovascular fitness. The term “cardiovascular” refers to both the heart and blood vessels. Since the health of the respiratory system is so closely linked to that of the blood circulation, fitness of both will be referred to as “cardiorespiratory”. During your fitness assessment, stop any test immediately if you begin to feel any pain, faintness, or dizziness. If you notice any other disturbing sensations such as headache or inability to get enough air, do not complete the test. DETERMINING TARGET HEART RATE ZONE If your heart rate becomes faster during physical activity, that exercise would be described as aerobic. These activities, when performed often enough and at long enough durations, result in increased efficiency of the circulatory and respiratory systems. The noted improvements are described as the training effect. The training effect has occurred if the heart rate is lower for a given type of exercise or if it takes more resistance to achieve the same heart rate. In order to experience the training effect and improved cardiorespiratory health, the exercise duration should exceed twenty continuous minutes and the heart rate should be within the target heart rate zone. There are numerous formulae that have been developed to determine an individual’s target heart rate. The range should
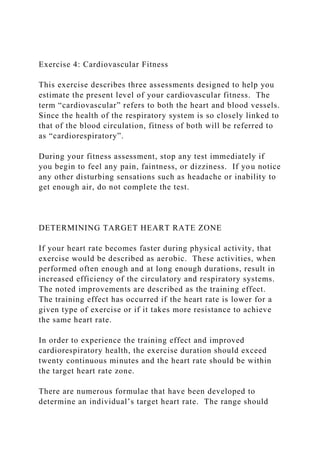
- 2. ensure sufficient stress to result in improvement, yet not exceed what would be safe. The formula that follows is based on age and resting heart rate. Resting heart rate is a simple way to assess current level of cardiorespiratory fitness. The average resting heart rate for healthy adults is 75, and ranges from 60-100 BPM (beats per minute). Well-conditioned endurance athletes have resting rates in the 30s and individuals with poor fitness would exhibit resting rates that are much higher. Powerful hearts and lungs circulate more oxygen per beat and can maintain the body at rest with fewer beats per minute. True resting heart rate is a value that stays constant for days, weeks, and longer, unless cardiovascular changes take place. When measuring HR for these exercises, make sure to record it when you are truly at rest. This will be the lowest value that you record. Use the calculations in Figure 5.1 as a guide to determine your personal target heart rate zone. Your heart rate should be within these limits whenever you participate in aerobic activities. Calculations should be revisited from time to time as resting heart rate will change with advancing age and, more frequently, due to effects of lifestyle changes. MinimumMaximum Maximum heart rate in healthy adult: 220 220 Subtract your age -20-20
- 3. 200 200 Subtract resting heart rate - 60- 60 140 140 Multiply by Lower and upper limit % .70.85 98 119 Add back resting heart rate +60 +60 Target heart rate zone (BPM) 158 179 Figure 4.1. Target heart rate zone calculations for a 20 year old with a RHR of 60 BPM. You will be measuring your heart rate by taking your pulse with your fingers. There are multiple locations on the surface of the body that can be used as pulse sites. The most commonly used arteries are the carotid and radial. Pulse sites, also known as pressure points, are depicted in Figure 5.2. Pulse is recorded by gently pressing on the arterial wall with fingers.
- 4. Figure 4.2. Pulse sites. ASSESSMENT #1 - EXERCISE RECOVERY RATE 1. Sit quietly for 10 minutes and measure your resting heart rate. 2. Jog in place or perform another aerobic exercise until your heart rate reaches the minimum target heart rate 5 beats. 3. Continue to exercise at the same stress level for 3 minutes. Don’t allow your heart rate to drop below the lower target heart rate or exceed the maximum target heart rate 5 beats. 4. Measure your heart rate during the last 15 seconds of exercising. 5. Measure your heart rate at 1-minute intervals until the rate is below 100 bpm. This is your recovery rate. If your recovery rate exceeds 5 minutes, your cardiovascular fitness is considered below average. ASSESSMENT #2 - HARVARD STEP TEST 1. Step on a step first with one foot and then with the other foot until you are standing with the knees unbent. Then step down with one foot followed by the other foot to return to the starting position. 2. Step at a pace that results in approximately 30 times per minute for a 5-minute period.
- 5. 3. Sit down and rest. Measure your heart rate 1 minute after exercising. Remain sitting and measure your heart rate at the 2- minute and 3-minute intervals after exercising. 4. Calculate the sum of the 3 heart rate values. Use this formula to calculate a fitness index: Fitness Index = 30,000 Sum of the Three Heart Rates Fitness Index Rating <55 Poor 55 – 64 Low average 65 – 69 Average 70 – 79 High average 80 – 89 Good 90 and above Excellent Figure 4.3. Harvard step test fitness index. ASSESSMENT #3 - THREE-MINUTE SIT-AND-STAND TEST 1. Sit quietly for 10 minutes and measure your resting heart rate. 2. Starting from a sitting position with arms folded across your chest, stand up and sit down at a rapid but comfortable pace.
- 6. Do this for three minutes. Your legs must be straight before you sit down and you must sit down completely. Do not use a chair with wheels. 3. Measure your heart rate during the last 15 seconds of exercising 4. Sit down and rest. Measure your heart rate at 30 seconds, 1 minute, and 2 minutes after you sit down. 5. Circle your resting, exercise, and 3 post-exercise heart rates in Table 5.1. Record the corresponding values written in bold in the first column of the table. Resting Exercise 30 Sec 1 Min 2 Min 20 44 80 64 56 56 19 48 84 68 60 60 18 52
- 9. 136 120 112 112 5 84 140 124 116 116 4 88 144 128 120 120 3 92 148 132 124 124 2 96 152 136 128 128 1 100 156 140 132 132 Table 4.1. Three-minute sit-and-stand fitness rating.
- 10. 6. Calculate the sum of the values for the 5 heart rates. If the sum is 0 – 35, your cardiovascular fitness is considered to be dangerously poor. Your cardiovascular fitness is average when the sum is 36 – 70. When the sum exceeds 70, your cardiovascular fitness is excellent. Lab Report Report the results of all three assessments. These can be done on yourself or any adult subject who volunteers. However, all three assessments should be done for the same individual. Your report should include (1) calculations for the subject’s target heart rate zone, (2) recorded heart rates as indicated in all charts and tables, (3) verbal (in sentence form) fitness descriptions for all three assessments, and (4) a general discussion of the results. Are the results consistent among the tests? Can you draw any conclusions based on relationships between fitness and other lifestyle parameters? Is the subject a smoker, overweight, or an active, fit person? A minimum of two photographs is required. These should depict the general appearance of your subject and the subject engaged in at least one of the fitness assessments. Your HCC Hawk Card or some other form of photo ID needs to be within every image. The ID should be on or near the subject when you take the picture.
- 11. The chair used for the sit-and-stand test needs to be sturdy and not upholstered, on casters (wheels) or a folding chair. Assessments should be completed either on different days or with a minimum of an hour between tests. This is necessary to remove fatigue as a possible explanation for diminished performance. 6 Assessment 2014, Vol. 21(1) 82 –91 © The Author(s) 2012 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/1073191112436665 asm.sagepub.com Traditional social science theories frequently offer single- variable explanations for complex behaviors. This is par- ticularly true of efforts to explain crime. Crime has been ascribed to social disadvantage, family structure, peer rela- tions, opportunity, and a host of other factors but only occa- sionally (e.g., Thornberry, 1987) do we see serious attempts to integrate these concepts. For research, policy, and clini- cal reasons, the desire on the part of many in the field to have an integrated perspective is strong. In fact, three of the most currently popular theories of crime, Moffitt’s (1993) dual trajectory model, Gottfredson and Hirschi’s (1990) self-control model, and Sampson and Laub’s (1993) age- graded life-course model of informal social control, have
- 12. sought to integrate traditional sociological concepts with principles from biology, psychology, and economics, respectively. Despite these promising developments, the field of criminology remains a field dominated by single- variable theories. As such, it has a long way to go before it can offer a broad-based integrated perspective on crime. It is my contention that greater progress could be made toward developing a broad-based integrated perspective on crime if scholars working in the fields of criminology and criminal justice would examine moderating and mediating effects between variables from different models. When discussing moderator and mediator variables the first order of business is properly defining the terms because they are often confused with each other even though they represent two distinct processes. As outlined in a classic paper by Baron and Kenny (1986), a moderator affects the direction or strength of the relationship between an inde- pendent or predictor variable and a dependent or outcome variable, whereas a mediator accounts, in part or in whole, for the relationship between an independent or predictor variable and dependent or outcome variable. To say that race moderates the criminal thinking–recidivism relation- ship means that the criminal thinking–recidivism rela- tionship is weaker or reversed for some races than others (e.g., Caucasian vs. African American). To say that educa- tion mediates the race–recidivism relationship means that education accounts, at least in part, for the race–recidivism 436665ASM21110.1177/10 73191112436665WaltersAssessment © The Author(s) 2012 Reprints and permissions: sagepub.com/journalsPermissions.nav
- 13. 1Federal Correctional Institution–Schuylkill, P.O. Box 700, Minersville, PA 17954, USA 2Kutztown University, Kutztown, PA, USA Corresponding Author: Glenn D. Walters, Department of Criminal Justice, Kutztown University, Kutztown, PA 19530-0730, USA. Email: [email protected] Relationships among Race, Education, Criminal Thinking, and Recidivism: Moderator and Mediator Effects Glenn D. Walters1,2 Abstract Moderator and mediator relationships linking variables from three different theoretical traditions—race (subcultural theory), education (life-course theory), and criminal thinking (social learning theory)—and recidivism were examined in 1,101 released male federal prison inmates. Preliminary regression analyses indicated that racial status (White, Black, Hispanic) moderated the relationship between criminal thinking, as measured by the General Criminal Thinking (GCT) score of the Psychological Inventory of Criminal Thinking Styles (PICTS), and recidivism. Further analysis, however, revealed that it was not racial status, per se, that moderated the relationship between the PICTS and recidivism, but educational attainment. Whereas the PICTS was largely effective in predicting recidivism in inmates with 12 or more years of education, it was largely ineffective in predicting recidivism in inmates with fewer than 12 years of education. When education and
- 14. the GCT score were compared as possible mediators of the race–recidivism relationship only the GCT successfully mediated this relationship. Sensitivity testing showed that the GCT mediating effect was moderately robust to violations of the sequential ignorability assumption on which causal mediation analysis rests. Moderator and mediator analyses are potentially important avenues through which theoretical constructs can be integrated and assessment strategies devised. Keywords race, education, criminal thinking, recidivism, moderation, mediation Article http://crossmark.crossref.org/dialog/?doi=10.1177%2F10731911 12436665&domain=pdf&date_stamp=2012-02-11 Walters 83 relationship through a causal chain of events that runs from race to education to recidivism. The purpose of the current study was to examine moderator and mediator relationships between concepts from three different theories of crime— race (subcultural theory), education (life-course theory), and criminal thinking (social learning theory)—and recidi- vism as a means of demonstrating how these constructs might be integrated for both theoretical and research purposes. Whether crime is assessed with official arrest records or offender self-report, African American men are more often arrested, convicted, and incarcerated for crime, and more often report criminal involvement than their European
- 15. American counterparts (Federal Bureau of Investigation, 2010; Sampson & Wilson, 1995). Rates of recidivism tend to be higher and survival times lower in African American men when African American men and European American men are compared (Jung, Spjeldnes, & Yamatani, 2010; Sabol, Minton, & Harrison, 2007). Black–White differ- ences in crime are particularly pronounced when analyses are restricted to more serious offenses (Piquero & Brame, 2008). Research further indicates that Hispanics commit fewer crimes than Blacks but significantly more crimes than Whites (Steffensmeier, Feldmeyer, Harris, & Ulmer, 2011). In all likelihood, the race–crime relationship is driven by a combination of cultural, structural, and social psychological factors, but it remains a central feature of several criminological theories, to include culture conflict theory (Sellin, 1938), social disorganization theory (Burgess & Bogue, 1967), and, most particularly, Wolfgang and Ferracuti’s (1967) subculture of violence perspective. Education has also been found to correlate with recidi- vism and is considered a criminogenic need capable of sig- nificantly reducing an adult or juvenile offender’s future chances of offending (Vieira, Skilling, & Peterson-Badali, 2009). In their age-graded life-course theory of offending, Sampson and Laub (1993) discuss the role of marriage, military service, employment, and education in transition- ing youthful offenders away from crime during late adoles- cence and early adulthood. According to Sampson and Laub (1993), these life-course changes have the power to divert a youthful offender from a criminal trajectory to a noncriminal trajectory. Hence, educational achievement should be capable of reducing future recidivism. Results from a series of recent studies, in fact, suggest that educa- tional attainment during incarceration is associated with a significantly lower rate of recidivism as well as a significant reduction in the seriousness of subsequent offenses
- 16. (Blomberg, Bales, Mann, Piquero, & Berk, 2011). School attendance was particularly beneficial to African American males but was effective in preventing future criminality across all racial and gender groups (Blomberg, Bales, & Piquero, 2012). In contrast to the sociological bent of most criminologi- cal theories, the social learning model takes a decidedly psychological approach to crime. With an emphasis on individual psychology rather than group process, social learning theory considers crime a function of observa- tional learning, covert reinforcement, and cognitive medi- ation. As part of his social learning–influenced criminal lifestyle model, Walters (2012) proposes the existence of six cognitive mediators (criminal thinking styles, attribu- tions, outcome expectancies, efficacy expectancies, goals, and values). These cognitive variables are held to mediate important relationships between crime-relevant variables. Using the General Criminal Thinking (GCT) score from the Psychological Inventory of Criminal Thinking Styles (PICTS: Walters, 1995) as a measure of criminal thinking, Walters (2009, 2011b, 2011c) has shown that the PICTS is capable of predicting recidivism after age and criminal history had been controlled. It is important for both theo- retical and practical reasons to understand if status vari- ables such as race and gender moderate this relationship and whether the GCT mediates important relationships between social status variables and recidivism. The first goal of this study was to evaluate whether race moderates the relationship between criminal thinking and recidivism. In other words, is the criminal thinking–recidi- vism relationship invariant across race? Although research has failed to identify consistent PICTS score differences between Black, White, and Hispanic inmates (Walters, 2002), there is some indication that race may moderate the
- 17. relationship between the PICTS and release outcome because recidivism is most effectively predicted in White inmates and least effectively predicted in Hispanic inmates (Walters, 1997; Walters, Frederick, & Schlauch, 2007). As a self-report measure, the PICTS requires a sixth- grade reading level or higher to complete. Education— which tends to be lower in Black and Hispanic inmates than in White inmates (Harlow, 2003)—and not race, may there- fore be responsible for moderating the relationship between the PICTS and recidivism. The second goal of this study was to evaluate whether education and the PICTS mediate the relationship between race and recidivism. Using causal mediation analysis and sensitivity testing (Imai, Keel, & Tingley, 2010), the mediating effect of both education and the GCT score on the race-recidivism relationship were evaluated. Method Participants The current sample was composed of 1,101 male inmates released from prison less than 42 months after providing a valid PICTS at a medium security federal correctional 84 Assessment 21(1) institution. At the time of their release, participants ranged in age from 19 to 78 years (M = 35.71, SD = 9.81) and had between 3 and 20 years of education (M = 11.33, SD = 1.94). More than two thirds of the sample was Black (68.1%), with the remainder of the sample consisting of White (19.6%), Hispanic (11.5%), and Asian/Native American (0.8%) par- ticipants. Nearly three quarters of the sample listed their marital status as single (73.3%), whereas 19.5%, 6.6%, and
- 18. 0.5% listed their marital status as married, divorced, and widowed, respectively. The two most common instant offenses in the current sample were drugs (27.5%) and parole/supervised release violations (27.1%); the remain- der of the sample was serving time for weapons violations (16.3%), robbery (9.3%), violent crimes (5.3%), property crimes (4.3%), and miscellaneous offenses (10.2%). Psychological Inventory of Criminal Thinking Styles The PICTS (Walters, 1995) is an 80-item self-report mea- sure designed to assess the eight thinking styles believed to support a criminal lifestyle. Each PICTS item is scored on a 4-point Likert-type scale (strongly agree, agree, uncer- tain, disagree), with strongly agree responses being assigned four points, agree responses three points, uncer- tain responses two points, and disagree responses one point on all scales except Defensiveness-revised (Df-r) where items are reverse-scored (strongly agree = 1, agree = 2, uncertain = 3, disagree = 4). The PICTS yields two 8-item validity scales—Confusion-revised (Cf-r) and Df-r—eight 8-item nonoverlapping thinking style scales—Mollification (Mo), Cutoff (Co), Entitlement (En), Power Orientation (Po), Sentimentality (Sn), Superoptimism (So), Cognitive Indolence (Ci), and Discontinuity (Ds)—four factor scales—Problem Avoidance (PRB), Infrequency (INF), Self-Assertion/Deception (AST), and Denial of Harm (DNH)—two composite scales—Proactive Criminal Thinking (P) and Reactive Criminal Thinking (R)—and a General Criminal Thinking (GCT) score. The GCT score, which is the sum of the raw scores for the eight PICTS thinking style scales, served as the criterion for criminal thinking in the current investigation. Research indicates that the GCT is an internally consistent (α = .95) measure with strong test-retest reliability (r = .84-.86, after 12 weeks), and moderate predictive validity (unweighted
- 19. mean r with recidivism = .22: Walters, 2002). Procedure The base sample from which data used in the current study were drawn contained 3,039 male inmates who had com- pleted the PICTS between 2003 and 2010 as part of a rou- tine intake screening procedure held in a medium security federal correctional institution in the northeastern United States. Nearly half the base sample (n = 1,435, 47.2%) had been released from prison at some point during the follow- up. In light of research showing that the predictive efficacy of the PICTS drops off when the test-release interval (number of months between completion of the PICTS and release from prison) exceeds 41 months (Walters, 2011c), 132 inmates with test-release intervals greater than 41 months were removed from the sample. One hundred and forty inmates who spent fewer than 12 months in the com- munity and showed no evidence of recidivism and 62 inmates who produced invalid PICTS profiles (20 or more unanswered items, Cf-r ≥ T-score of 95, or Df-r ≥ T-score of 68; Walters, 2011c) were also eliminated from the study. This resulted in a final sample of 1,101 male inmates who recidivated during the follow-up or were recidivism-free for at least 12 months in the community. The independent (predictor) variable for the moderator analyses was the PICTS GCT score. Race (White and Asian/Native American = 1, Black = 2, Hispanic = 3) and education (<12 years = 1, ≥12 years = 2) served as modera- tor variables. Recidivism constituted the dependent (out- come) variable. A review of electronic files from the Federal Bureau of Investigation’s National Crime Information Center and Federal Bureau of Prisons’ inmate data base were used to construct the recidivism outcome (yes = 1, no = 0). Technical parole violations were counted as evidence
- 20. of recidivism when they resulted in the individual’s return to prison. Nearly two thirds of the sample (65.8%) received at least one charge. For the purposes of comparison and incremental validity, two additional predictor variables were included in some of the analyses: age at time of release from prison and the violation factor score from the Lifestyle Criminality Screening Form (LCSF-V; Walters, White, & Denney, 1991). The LCSF-V was employed as a proxy for criminal history in this study. Moderator analyses were conducted in two stages. In the first stage, the dichotomous recidivism outcome measure (Y) was regressed onto the GCT score (X), moderator vari- able (Z; either race or education), and GCT-moderator interaction (XZ) as part of a Cox survival regression analy- sis that considers both the recidivism event (0/1) and time until recidivism. If the interaction was significant, nonlinear quadratic terms (X2, Z2) were added to the equation and inserted before the interaction term and the analysis recom- puted (Cortina, 1993; Lubinski & Humphreys, 1990). In the second stage, receiver operating characteristic (ROC) curves were calculated separately for White, Black, and Hispanic inmates and for inmates with less (<12 years) and more (≥12 years) education. ROC analyses were also calculated for inmates with less and more education within each of the three racial groups. Cox regression analyses were also used to test the incremental validity of the GCT relative to age at Walters 85 time of release and criminal history (LCSF-V). These anal- yses were conducted separately for each educational level (<12 years, ≥12 years) in the full sample as well as in each of the three racial subsamples.
- 21. A mediation analysis was conducted with race (White and Asian/Native American = 1, Black and Hispanic = 2) as the independent variable, recidivism as the dependent (out- come) variable, and education and GCT each considered as mediator variables. Given the prospective nature of the current design (i.e., race preceded education/GCT and education/GCT preceded recidivism) a mediation analysis was justified. Causal mediation analysis was performed with algorithms devised by Imai and his colleagues (Imai, Keel, & Tingley, 2010; Imai, Keel, Tingley, & Yamamoto, 2010). The (continuous) mediator models (education, criminal thinking) were fit with linear least squares regression and the (binary) outcome model (recidivism) was fit with probit regression. After completing Step 1 of the procedure, output objects were bootstrapped 1,000 times with replacement using a nonparametric mediational analysis. Sensitivity to violations of the sequential ignorability assumption (absence of confounders that could explain the mediation results) was tested with a sensitivity analysis of the mediation and outcome models using two covariate confounders: age (in years) and the LCSF-V score. Results Descriptive statistics for and intercorrelations between the three theoretical variables (race, education, GCT) and the single-outcome measure (recidivism) are provided in Table 1. As the results indicate, all three theoretical variables cor- related significantly among themselves and each predicted recidivism. Moderator Analyses Table 2 summarizes the results of the first set of moderator analyses. Cox regression analysis of race as a moderator variable revealed a significant interaction between the PICTS GCT score and race (left column of Table 2). When
- 22. nonlinear quadratic terms (X2, Z2) were added to the equa- tion, the PICTS GCT effect remained significant (Wald = 5.43, p < .05) but the interaction became nonsignificant (Wald = 3.60, p = .06). Replacing race with education as the moderator of the GCT–recidivism relationship resulted in a Cox regres- sion analysis in which none of the main effects (GCT, education) or the interaction effect (education × GCT) achieved statistical significance (right column of Table 2). It should be noted, however, that before the interaction term was introduced into the model, both the GCT (Wald = 33.19, p < .001) and education (Wald = 4.27, p < .05) main effects were significant. At first glance, these results seem consis- tent with the conclusion that race exerted a moderating effect on the GCT–recidivism relationship in this study. Further analysis, however, revealed that the significant interaction between race and the GCT became nonsignifi- cant when quadratic terms were added to the estimated model and that although education did not achieve a statis- tically significant interaction with GCT, inclusion of the education × GCT interaction term eliminated a highly sig- nificant GCT effect, something the race × GCT interaction failed to do even when quadratic terms were added to the model. To further investigate the ability of race and education to moderate the GCT–recidivism relationship, ROC analyses were computed by race (White, Black, Hispanic) and edu- cation (<12 years, ≥12 years). As the results outlined in Table 3 indicate, the GCT score achieved the most accurate results with White participants, the least accurate results Table 1. Descriptive Statistics and Correlations for the Three Predictors and Recidivism Outcome. Correlations
- 23. Predictor Mean SD Range Education GCT Recidivism Race 1.80 0.40 1-2 −.15** .11** .12** Education 11.33 1.94 3-20 −.12** −.08* PICTS GCT 113.85 27.20 67-217 .17** Recidivism 0.66 0.48 0-1 Note. Race = White (1) versus Black or Hispanic (2); Education = years of education; PICTS GCT = General Criminal Thinking score of the Psychological Inventory of Criminal Thinking Styles; SD = standard deviation; Range = high and low scores on this particular measure in the current sample; N = 1101. *p < .01. **p < .001. Table 2. Summary of Cox Regression Results With Race and Education as Moderator Variables. Race moderator Education moderator Predictor Wald [95% CI] Wald [95% CI] PICTS GCT 21.85** 1.02 [1.012, 1.029] 0.26 1.00 [0.993, 1.011] Moderator 8.51* 2.09 [1.275, 3.442] 2.79 0.58 [0.308, 1.099] Moderator × GCT 8.73* 0.99 [0.990, 0.998] 2.38 1.00 [0.998, 1.009]
- 24. Note. Figures reported are the final logistic regression results at the end of Block 2; Predictor = predictor variables; PICTS GCT = General Criminal Thinking score of the Psychological Inventory of Criminal Thinking Styles; Moderator = moderator variable, either race (White = 1, Black = 2, Hispanic = 3) or education (1 = less than 12 years, 2 = 12 or more years); Moderator × GCT = moderator (either race or education) by GCT interaction; Wald = Wald statistic with a χ2 distribution and one degree of freedom; exp(β) = exponent of the unstandardized coefficient in the form of an odds ratio (numbers below 1.00 indicate a negative relationship with the criterion and numbers above 1.00 indicate a positive relationship with the criterion); 95% CI = 95th percentile confidence interval for the exponent of the estimated coefficient; N = 1101. *p < .01. **p < .001. exp( )βx s exp( )βx s 86 Assessment 21(1) with Hispanic participants, and intermediate results with Black participants. A z-test procedure designed to compare independent ROC curves, nonetheless, failed to detect any
- 25. significant differences in the area under the curve (AUC) results between Blacks and Whites, z = 0.87, p > .10, Blacks and Hispanics, z = 1.04, p > .10, or Hispanics and Whites, z = 1.58, p > .10. A significant difference in accuracy did arise, however, when higher and lower educated partici- pants were compared, z = 2.20, p < .05. A z-test comparison of dependent ROC curves revealed that the PICTS GCT score was significantly more accurate in predicting recidi- vism in higher educated participants than age at time of release, z = 2.14, p < .05, and the LCSF-V was significantly more accurate than the GCT in predicting recidivism in lower educated participants, z = 2.40, p < .05. A second round of Cox regression analyses were con- ducted using all three indicators (age at time of release, LCSF-V, PICTS GCT) as predictors for the purpose of determining whether the PICTS GCT score possessed incremental validity relative to age and the LCSF-V. When the analyses were restricted to inmates with higher educa- tional levels, the GCT score displayed incremental validity relative to age at time of release and LCSF-V (left half of Table 4). When the analyses were restricted to inmates with lower educational levels, the GCT score failed to achieve incremental validity relative to age at time of release and the LCSF-V (right half of Table 4). When these analyses were conducted on the three racial groups separately, the GCT score achieved incremental validity relative to age and the LCSF-V in White (Wald = 8.39, p < .01) and Black (Wald = 14.24, p < .001) inmates with higher educational levels but not in White (Wald = 2.20, p >.10) and Black (Wald = 3.31, p =.07) inmates with lower educational levels. Although the GCT score failed to demonstrate incre- mental validity in either higher (Wald = 1.07, p > .10) or lower (Wald = 0.55, p > .10) educated Hispanic partici- pants, the beta value was in the predict direction (positive)
- 26. in the higher educated Hispanic group and in the nonpre- dicted direction (negative) in the lower educated Hispanic group. Table 3. Receiver Operating Characteristic Results by Race and Educational Level. Description N % Invalid GCT Age LCSF-V Total sample 1,101 5.3 .604 [.569, .639]** .595 [.560, .630]**; .612 [.576, .647]** Education ≥ 12 672 4.4 .628 [.584, .671]** .565 [.521, .609]* .592 [.548, .636]** Education < 12 429 6.7 .546 [.488, .605] .618 [.558, .677]** .645 [.584, .706]** White 224 4.8 .640 [.568, .713]** .621 [.547, .695]* .603 [.528, .678]* Education ≥ 12 170 4.6 .658 [.577, .740]** .579 [.492, .665] .605 [.520, .690]* Education < 12 54 5.7 .540 [.373, .707] .691 [.534, .848]* .591 [.425, .757] Black 750 5.1 .602 [.557, .646]** .572 [.528, .616]* .591 [.546, .636]** Education ≥ 12 448 4.5 .618 [562, .674]** .553 [.498, .608] .576 [.520, .632]* Education < 12 302 5.9 .558 [.484, .632] .578 [.502, .655]* .613 [.533, .693]* Hispanic 127 7.3 .543 [.442, .644] .668 [.574, .762]** .638 [.542, .735]* Education ≥ 12 54 1.8 .619 [.467, .771] .587 [.432, .741] .523 [.366, .679] Education < 12 73 11.0 .499 [.365, .633] .714 [.592, .835]* .706 [.584, .827]* Note. Description = description of sample in terms of race (White, Black, Hispanic) and education (12 or more years, less
- 27. than 12 years); N = sample or subsample size; % Invalid = proportion of Psychological Inventory of Criminal Thinking Styles (PICTS) that were removed because they were invalid; GCT = PICTS General Criminal Thinking score; Age = age at time of release (inverse scored); LCSF-V = Violation factor of the Lifestyle Criminality Screening Form; the first number in the GCT, Age, and LCSF-V columns is the area under the ROC curve (AUC) and the next set of numbers [in brack- ets] is the 95% confidence interval of the AUC. *p < .05. **p < .001. Table 4. Summary of Incremental Validity Cox Regression Analyses for Inmates With ≥12 Years of Education and for Inmates With <12 Years of Education. Education ≥ 12 years (n = 672) Education < 12 years (n = 429) Predictor Wald exp( )βx s [95% CI] Wald exp( )βx s [95% CI]
- 28. Age 6.95* 0.87 [0.78, 0.96] 15.45** 0.78 [0.69, 0.88] LCSF-V 22.69** 1.27 [1.15, 1.40] 16.85** 1.25 [1.12, 1.38] PICTS GCT 21.70** 1.24 [1.13, 1.36] 2.93 1.10 [0.99, 1.24] Note. Figures reported are the final logistic regression results at the end of Block 2; Predictor = predictor variables; Age = age at time of release from prison; LCSF-V = violation factor of the Lifestyle Criminality Screening Form; PICTS GCT = General Criminal Thinking score of the Psychological Inventory of Criminal Thinking Styles; Wald = Wald statistic with a χ2 distribution and one degree of freedom; exp(β) = exponent of the x-standardized (M = 0, SD = 1) coefficient in the form of an odds ratio (numbers below 1.00 indicate a negative relationship with the cri- terion and numbers above 1.00 indicate a positive relationship with the criterion); 95% CI = 95th percentile confidence interval for the exponent of the estimated coefficient. *p < .01. **p < .001. Walters 87 Mediator Analyses In causal mediation analysis a significant mediating effect is defined by a 95% confidence interval that does not include zero (Imai, Keel, & Tingley, 2010; Imai, Keel,
- 29. Tingley, et al., 2010). As indicated by the results in Table 5, education failed to mediate the relationship between race and recidivism. The GCT score, on the other hand, success- fully mediated the race-recidivism relationship (see Table 6). Further analysis revealed that the mediating effect of the GCT score on the race-recidivism relationship was only partial (direct effect still significant) and that it accounted for approximately 15% of the total variance in this relation- ship. When the GCT score was used to mediate the education– recidivism relationship the total model effect failed to achieve significance (95% confidence interval = −0.0142 to 0.0045). Sensitivity testing was performed on the mediation and outcome models using age and the LCSF-V score as confounding covariates. The results indicated a rho (ρ) at which mediation equals zero of .16 (see Figure 1). Coefficients of determination (R2) for the mediator and out- come models were used to construct a graph of the amount of variance that an unobserved confounder would have to explain to totally eliminate the mediation effect of GCT on the race–recidivism relationship (see Figure 2). According to the graph, an unobserved confounding variable or set of variables would need to account for approximately 14% of the variance in the mediator and 14% of the variance in the outcome to reduce the mediation effect to zero. Regression analyses in which GCT was regressed onto age and the LCSF-V score revealed an R2 of .018 (media- tion model) whereas logistic regression analyses in which recidivism was regressed onto age and the LCSF-V pro- duced a pseudo-R2 of .067 (outcome model). Only the bino- mial logistic regression results (outcome model) exceeded the minimum requirements for explaining recidivism (R2 ≥ .035) or GCT (R2 ≥ .04), and even then the amount of
- 30. mediator variance required to bring the mediation effect down to zero would have had to have been more than 45%. Instead, the two covariate confounders accounted for only 1.8% of the variance in the mediator variable. Discussion The results of this study suggest that testing for moderation and mediation can be helpful in integrating concepts from different theories. Patterns of moderation and mediation Table 5. Results of a Causal Mediation Analysis in Which Education Served as a Mediator of the Race–Recidivism Relationship. Effect type Point estimate 95% CI Mediation effect (Race → Educ → Recid) 0.0051 [−0.0043, 0.0157] Direct effect (Race → Recid) 0.0968 [0.0244, 0.1699] Total effect 0.1019 [0.0299, 0.1713] Proportion of total effect via mediation 0.0494 [0.0297, 0.1627] Note. Race = White (1) versus non-White (2). Educ = education
- 31. (in years); Recid = recidivism (yes = 1, no = 0); Point Estimate = estimate of the size of the effect; 95% CI = 95% confidence interval of the point estimate; N = 1101. Table 6. Results of a Causal Mediation Analysis in which General Criminal Thinking Served as a Mediator of the Race- Recidivism Relationship. Effect type Point estimate 95% CI Mediation effect (Race → GCT → Recid) 0.0159 [0.0053, 0.0294] Direct effect (Race → Recid) 0.0906 [0.0173, 0.1592] Total effect 0.1066 [0.0362, 0.1783] Proportion of total effect via mediation 0.1477 [0.0887, 0.4288] Note. Race = White (1) vs. non-White (2). Educ = education (in years); Recid = recidivism (yes = 1, no = 0); Point estimate = estimate of the size of the effect; 95% CI = 95% confidence interval of the point estimate; N = 1,101.
- 32. -1.0 -0.5 0.0 0.5 1.0 ACME(ρ) Sensitivity Parameter: ρ A ve ra ge M ed ia tio n E ffe ct : δ (t ) 0. 2 0. 2 0.
- 33. 1 0. 1 0. 0 Figure 1. Sensitivity analysis of the binary recidivism outcome and continuous criminal thinking mediator. The dashed line represents the estimated mediation effect, the solid line represents the estimated average mediation effect at different levels of ρ, and the gray region represents the 95% confidence interval for estimated average mediation effect at different levels of ρ. 88 Assessment 21(1) may provide clues as to how different concepts might fit together in an integrated theory. A concept central to life- course theory (educational attainment), for instance, moderated the criminal thinking–recidivism relationship whereas a concept central to subcultural theory (race) did not. Likewise, a concept central to social learning theory (criminal thinking) mediated the race–recidivism relation- ship whereas educational attainment did not. In the modera- tor analyses, the GCT score was able to predict recidivism in individuals with 12 or more years of education but it failed to predict recidivism in individuals with fewer than 12 years of education. Because 61% of the current sample had 12 years or more of education and more than two thirds
- 34. of samples such as the present one dropped out of high school prior to completing the 12th grade (Walters et al., 1991), a substantial portion of participants in the current study probably earned their GEDs in prison. Educational attainment in prison has been found to exert a protective effect against future recidivism (Blomberg et al., 2011); and in the current study, it displayed a moderating effect on the GCT–recidivism relationship but failed to mediate the race–recidivism relationship. If one follows the logic that interaction between an inde- pendent variable and putative moderator variable in a regression equation equals a moderator effect, then race moderated the criminal thinking–recidivism relationship in this study. However, when nonlinear monotonic terms for the independent and moderator variables (X2 and Z2) were included in the regression equation (Cortina, 1993; Lubinski & Humphreys, 1990), the previously significant interaction effect turned nonsignificant. In addition, even though the education × GCT interaction failed to achieve statistical significance in this study, the inclusion of this interaction term in the regression equation completely eliminated an effect for GCT that had been significant without the interac- tion. Further analyses were accordingly conducted for the purpose of disentangling the possible confounding effect of education on race. In these analyses, AUC values were cal- culated for subgroups divided by race (White, Black, Hispanic) and education (<12 years, ≥ 12 years). Rice and Harris (2005) have determined that an AUC of .556 is com- parable to a small effect size, an AUC of .639 is comparable to a moderate effect size, and an AUC of .714 is comparable to a large effect size. Effect size estimates for individuals with 12 or more years of education were of low-moderate to moderate magnitude across all three racial conditions, whereas effect size estimates for individuals with fewer than 12 years education were of zero to small magnitude for
- 35. White, Black, and Hispanic respondents. These results indi- cate that education was the moderating variable in this study and that differences in efficacy across the three racial groups were an artifact of a greater proportion of Black (40.3%) and Hispanic (57.5%) than White (24.1%) inmates with fewer than 12 years of education. Whereas moderation provides information on the rela- tive stability or invariance of a relationship, mediation pro- vides information on the nature of a relationship. In the current study, criminal thinking was found to partially mediate the relationship between race and recidivism. Hence, criminal thinking was differentially associated with race and recidivism such that a portion of the relationship between race and recidivism was explained by criminal thinking. Other cognitive and noncognitive variables prob- ably also mediate the race–recidivism relationship. One recent study, in fact, confirmed that Black inmates had sig- nificantly more positive outcome expectancies for crime than White inmates (Walters, 2011a). Unfortunately, because there was no outcome variable (e.g., recidivism) in that study no conclusions about mediation can be drawn. Even so, Walters (2012) includes outcome expectancies and criminal thinking styles in his social learning theory of cog- nitive mediation. A study in which all six cognitive medi- ators (criminal thinking styles, attributions, outcome expectancies, efficacy expectancies, goals, and values) are considered simultaneously would provide more information on the role of cognitive mediation in the race–recidivism relationship. -0.08 -0.06 -0.04
- 36. -0.02 0 0.4 0.8 0. 0 0. 2 0. 4 0. 6 0. 8 1. 0 RM ~2 ACME(RMRY), sgn](λ2λ3) = 1 ~2 ~2 R Y ~2
- 37. 0. 1 0. 3 0. 5 0. 7 0. 9 0.0 0.1 0.2 0.3 0.5 0.6 0.7 0.9 1.0 Figure 2. Sensitivity analysis of the binary recidivism outcome and continuous criminal thinking mediator. Contour lines represent the estimated average mediational effect at different levels of an unobserved confounder. The “0” line indicates how strong the unobserved confounder must be to completely eliminate the mediation effect. Therefore, if the unobserved confounder accounts for 20% of the variance in the outcome (R̃ 2 y) then it must also account for at least 11% of the variance in the mediator (R̃ 2 M) to reduce the mediation
- 38. effect to zero. If the unobserved confounder accounts for 20% of the variance in the mediator (R̃ 2 M) then it would need to account for 10% of the variance in the outcome (R̃ 2 y) to reduce the mediation effect to zero. Walters 89 There are methodological, theoretical, practical, and policy implications to the current findings that need to be discussed. Methodologically, the current results indicate that equating interaction with moderation is problematic in several respects. First, there is the problem of Type I errors. As reported by Lubinski and Humphreys (1990) and others (Cortina, 1993; Ganzach, 1997), a spurious interaction effect can surface if quadratic terms are not added to the regression equation. In the current study, the significant race × GCT interaction disappeared once quadratic terms for the independent and moderator variables were added to the model. Second, there is the problem of Type II errors. Whereas a Type I error entails rejecting a null hypothesis that is true, a Type II error involves failing to reject a null hypothesis that is, in fact, false. Interaction has been known to suffer from low power (Cronbach, 1987; Lubinski & Humphreys, 1990). Adding quadratic terms to the estimated model can reduce the power of the interaction term even further (Cortina, 1993) and may be why the race × GCT interaction went from significant (p < .01) to nonsignificant (p = .06) after the quadratic terms had been added. Be this
- 39. as it may, dividing the sample along racial and educational lines made it clear that the chief moderating variable in the current study, even though it did not produce a significant interaction effect, was education. In testing mediation of the race–recidivism relationship I relied on a relatively new procedure development by Imai, Keel, & Tingley (2010) and Imai, Keel, Tingley, et al. (2010). Despite its recent arrival on the methodological scene, Imai et al.’s procedure is well documented and supported by mathematical proofs. In addition, it has the capacity for sensitivity testing, some- thing that is missing from most structured equation model- ing programs currently used to assess mediation effects. The current study also has implications for theory devel- opment. Given the plethora of single variable models in criminology the task of organizing and integrating these models into a single comprehensive theory is truly formi- dable. Integration could nonetheless be made easier with the aid of moderation and mediation analysis. In the current study, concepts central to three different criminological models—race (subcultural theories), education (life-course theories), and criminal thinking (social learning theories)— were integrated using moderation and mediation method- ologies. The results indicated that education but not race moderated the criminal thinking–recidivism relationship and that criminal thinking but not education mediated the race-recidivism relationship. Moderation and mediation analysis can be very useful in determining which constructs from various models belong together and which ones do not. The mediation analyses were particularly helpful in clarifying important criminological relationships. From the mediation results we can surmise that the effect of race on recidivism is at least partially mediated by cognitive factors such as criminal thinking, as well as, perhaps, by positive outcome expectancies for crime (Walters, 2011a), lower
- 40. investment in marriage (King & South, 2011), and social- environmental differences between Black and White Americans (Phillips, 2002; Sampson, Morenoff, & Raudenbush, 2005). Future research could further clarify important theoretical relationships by examining how these and other potential mediating variables interact to shape and influence the race–recidivism relationship. The current results, in addition to their methodological and theoretical implications, have potentially important practical implications, particularly for assessment. A self- report inventory is only as good as its ability to be compre- hended by those who complete it. The PICTS items were originally written to reflect a 6th-grade reading level but subsequent analyses have shown that some of the items require as much as a 9th- or 10th-grade reading level (Walters, 2002). Completing 12 years of education or receiv- ing a GED were proxies for a sufficient level of reading ability in the current study. Most of the inmates who partici- pated in this study (61%) attained one of these two markers and were effectively classified for recidivism risk at a low- moderate to moderate level by the PICTS GCT score. The remaining 39% of the sample, however, could not be effec- tively classified for recidivism risk based on the results of the PICTS GCT score. These findings lead to the following two conclusions. First, we must rely more on demographic and historical measures such as age and the LCSF-V and less on self-report measures such as the PICTS when evalu- ating individuals with limited educational attainment and reading ability. Second, for the PICTS to be effective with a larger segment of the inmate population, the item content may need to be revised so that individuals with less than a 12th-grade education or 9th-grade reading level can com- prehend the items sufficiently well enough to construct a valid protocol. Classification of offenders on the basis of race would be both illegal and unethical. The current results,
- 41. however, point to a factor (i.e., criminal thinking) that may be partially responsible for racial differences in recidivism and which could lay the groundwork for a more rationale and effective offender classification system. Both the moderation and mediation results from this study have implications for criminal justice policy and cor- rectional decision making. The policy implications of the moderating effect of education on the efficacy of the PICTS GCT score in predicting recidivism is that guidelines need to be established for the proper use of the PICTS in identify- ing criminogenic needs and assigning offenders to pro- grams and levels of supervision. Depending on the offender’s education or reading level, alternative proce- dures (criminal history and other static risk factors) may need to be employed for the purpose of making program and classification decisions. The policy implications of the race → criminal thinking → recidivism mediation effect is that it emphasizes the necessity of including a criminal 90 Assessment 21(1) thinking component in secondary and tertiary prevention programs for minority youth. Although criminal thinking is a criminogenic need in offenders of all races and at all ages (Andrews, Bonta, & Wormith, 2006), its mediating role in the race–recidivism relationship suggests that it may be a particularly salient goal for interventions with African American and Hispanic youth. Limitations A principal limitation of the moderator results of this study is that reading ability was not tested. If reading ability rather than education moderates the relationship between criminal
- 42. thinking, as measured by the PICTS GCT score, and recidi- vism, then additional research is required using a validated adult measure of reading comprehension such as the Adult Basic Learning Examination (ABLE) or Tests of Adult Basic Education (TABE). In addition, factors other than or in addi- tion to reading level may moderate the GCT–recidivism relationship. Motivation may be one such factor. Lack of motivation could lead someone to drop out of school as well as exert less than maximum effort on a psychological inven- tory. The GCT–recidivism relationship could consequently be moderated by reading ability, motivation, and other cor- relates of education, but not race. Understanding moderation is a little like peeling back the layers of an onion. Race rep- resents the outer layer of the onion, education the next layer, reading level and motivation the layer below this, and so on until we reach the core moderator v ariable(s). The mediation results also suffer from a significant limi- tation. The confounding covariates in the sensitivity analy- sis should predate the treatment (independent) variable. In the current study, the treatment or independent variable was race. Because race is present at birth it was not possible to find confounding covariates in the current database that preceded the independent variable. This is a limitation but not a fatal flaw of the mediation analysis. The use of pre- treatment confounders is based on the assumption that the independent and mediator variables were assigned ran- domly to participants. Using a nonmanipulated independent variable such as race will always raise questions about sequential ignorability. In the current study, the conditions for prospective analysis were satisfied—that is, the indepen- dent variable (race) preceded the mediating variable (GCT) that then preceded the dependent variable (recidivism)—and the two potential confounders (age and prior criminal his- tory as represented by the LCSF-V), although not predating the independent variable, did predate the mediator.
- 43. Moreover, in light of the fact that age and criminal history are often considered the two best predictors of recidivism (Gendreau, Little, & Goggin, 1996), potentially significant confounders of the race → GCT → recidivism mediated pathway were examined and found not to present a serious challenge to the robustness of the mediation effect. Sampling was a limitation that affected both the modera- tion and mediation analyses. Because participants in this study were incarcerated federal male offenders we do not know how well these results apply to nonincarcerated, state, or female offenders. Additional research is consequently required to test the generalizability of the current results to populations different from those included in the current study. Generalizability is also a limitation of the PICTS in the sense that it was only capable of effectively predicting recidivism in participants with 12 or more years of educa- tion. Lowering the reading level of some of the PICTS items should make the test more applicable to a larger por- tion of the inmate population, but it will never make it accessible to the entire inmate population. There will always be inmates who will need to be evaluated with demographic, historical, or behavioral indicators. This is a limitation inherent to all self-report measures of criminality, but it is a limitation we must endure if our goal is to assess criminal thinking. Author’s Note The assertions and opinions contained herein are the private views of the author and should not be construed as official or as reflect- ing the views of the Federal Bureau of Prisons or the United States Department of Justice.
- 44. Declaration of Conflicting Interests The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Glenn D. Walters is the author of the Psychological Inventory of Criminal Thinking Styles (PICTS) and receives remuneration from sales of the PICTS manual. Funding The author received no financial support for the research, author- ship, and/or publication of this article. References Andrews, D. A., Bonta, J., & Wormith, S. J. (2006). The recent past and near future of risk and/or need assessment. Crime & Delinquency, 52, 7-27. Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Concep- tual, strategic, and statistical considerations. Journal of Per- sonality and Social Psychology, 51, 1173-1182. Blomberg, T. G., Bales, W. D., Mann, K., Piquero, A. R., & Berk, R. A. (2011). Incarceration, education and transition from delinquency. Journal of Criminal Justice, 39, 355-365. Blomberg, T. G., Bales, W. D., & Piquero, A. R. (2012). Is educational
- 45. achievement a turning point for incarcerated offenders across race and sex? Journal of Youth and Adolescence, 41, 202-216. Burgess, E., & Bogue, D. J. (Eds.). (1967). Urban sociology. Chicago, IL: University of Chicago Press. Walters 91 Cortina, J. M. (1993). Interaction, nonlinearity, and multicol- linearity: Implications for multiple regression. Journal of Management, 19, 915-922. Cronbach, L. J. (1987). Statistical tests for moderator variables: Flaws in analyses recently proposed. Psychological Bulletin, 102, 414-417. Federal Bureau of Investigation. (2010). Crime in the United States: 2009. Washington, DC: Author. Ganzach, Y. (1997). Misleading interaction and curvilinear terms. Psychological Methods, 2, 235-247. Gendreau, P., Little, T., & Goggin, C. (1996). A meta-analysis of the predictors of adult offender recidivism: What works! Criminology, 34, 575-607. Gottfredson, M., & Hirschi, T. (1990). A general theory of crime. Stanford, CA: Stanford University Press. Harlow, C. W. (2003). Education and correctional populations [Bureau of Justice Statistics Special Report]. Washington,
- 46. DC: U.S. Department of Justice. Imai, K., Keele, L., & Tingley, D. (2010). A general approach to causal mediation analysis. Psychological Methods, 15, 309-334. Imai, K., Keele, L., Tingley, D., & Yamamoto, T. (2010). Causal medi- ation analysis using R. In H. D. Vinod (Ed.), Advances in social science research using R (pp. 129-154). New York, NY: Springer. Jung, H., Spjeldnes, S., & Yamatani, H. (2010). Recidivism and survival time: Racial disparity among jail ex-inmates. Social Work Research, 34, 181-189. King, R. D., & South, S. J. (2011). Crime, race, and the transition to marriage. Journal of Family Issues, 32, 99-126. Lubinski, D., & Humphreys, L. G. (1990). Assessing spurious “moderator effects”: Illustrated substantively with the hypoth- esized (“synergistic”) relation between spatial and mathemati- cal ability. Psychological Bulletin, 107, 385-393. Moffitt, T. E. (1993). Adolescence-limited and life-course persis- tent antisocial behavior: A developmental taxonomy. Psycho- logical Review, 100, 674-701. Phillips, J. A. (2002). White, black, and Latino homicide rates: Why the difference? Social Problems, 49, 349-374. Piquero, A. R., & Brame, R. W. (2008). Race-crime and ethnicity- crime relationship in a sample of serious adolescent delin-
- 47. quents. Crime & Delinquency, 54, 390-422. Rice, M. E., & Harris, G. T. (2005). Comparing effect sizes in follow-up studies: ROC area, Cohen’s d, and r. Law and Human Behavior, 29, 615-620. Sabol, W. J., Minton, T. D., & Harrison, P. M. (2007). Prison and jail inmates at midyear 2006 (NCJ 217675). Bureau of Justice Statistics Bulletin. Washington, DC: Bureau of Justice Statistics. Sampson, R. J., & Laub, J. H. (1993). Crime in the making: Path- ways and turning points through life. Cambridge, MA: Har- vard University Press. Sampson, R. J., Morenoff, J. D., & Raudenbush, S. (2005). Social anatomy of racial and ethnic disparities in violence. American Journal of Public Health, 95, 224-232. Sampson, R. J., & Wilson, W. J. (1995). Toward a theory of race, crime, and urban inequality. In J. Hagan & R. D. Peterson (Eds.), Crime and inequality (pp. 37-54). Stanford, CA: Stan- ford University Press. Sellin, T. (1938). Culture and conflict in crime. New York, NY: Social Science Research Council. Steffensmeier, D., Feldmeyer, B., Harris, C. T., & Ulmer, J. T. (2011). Reassessing trends in black violent crime, 1980-2008: Sorting out the “Hispanic effect” in Uniform Crime Reports arrests, National Crime Victimization Survey offender esti- mates, and U.S. prisoner counts. Criminology, 49, 197-251.
- 48. Thornberry, T. P. (1987). Toward an interactional theory of delin- quency. Criminology, 25, 863-892. Vieira, T. A., Skilling, T. A., & Peterson-Badali, M. (2009). Matching court-ordered services with offender needs: Predict- ing treatment success with young offenders. Criminal Justice and Behavior, 36, 385-401. Walters, G. D. (1995). The Psychological Inventory of Criminal Thinking Styles: Part I. Reliability and preliminary validity. Criminal Justice and Behavior, 22, 307-325. Walters, G. D. (1997). Predicting short-term release outcome using the LCSF and PICTS. Journal of Mental Health in Cor- rections Consortium, 43, 18-25. Walters, G. D. (2002). The Psychological Inventory of Criminal Thinking Styles (PICTS): A review and meta-analysis. Assess- ment, 9, 278-291. Walters, G. D. (2009). The Psychological Inventory of Criminal Thinking Styles and Psychopathy Checklist: Screening Ver- sion as incrementally valid predictors of recidivism. Law and Human Behavior, 33, 497-505. Walters, G. D. (2011a). Black-white differences in positive out- come expectancies for crime: A study of male federal prison inmates. Journal of Criminal Justice, 39, 192-197. Walters, G. D. (2011b). Predicting recidivism with the Psycholog- ical Inventory of Criminal Thinking Styles and Level of Ser- vice Inventory–Revised: Screening Version. Law and Human Behavior, 35, 211-220.
- 49. Walters, G. D. (2011c). Taking the next step: Combining incre- mentally valid indicators to improve recidivism prediction. Assessment, 18, 227-233. Walters, G. D. (2012). Crime in a psychological context: From career criminals to criminal careers. Thousand Oaks, CA: SAGE. Walters, G. D., Frederick, A. A., & Schlauch, C. (2007). Post- dicting arrests for proactive and reactive aggression with the PICTS proactive and reactive scales. Journal of Interpersonal Violence, 22, 1415-1430. Walters, G. D., White, T. W., & Denney, D. (1991). The Lifestyle Criminality Screening Form: Preliminary data. Criminal Jus- tice and Behavior, 18, 406-418. Wolfgang, M. E., & Ferracuti, E. (1967). Subculture of violence: Towards an integrated theory of criminology. London, England: Tavistock. Available online at www.sciencedirect.com ScienceDirect Comprehensive Psychiatry 55 (2014) 489–496 www.elsevier.com/locate/comppsych Mediators and moderators of functional impairment in adults with obsessive–compulsive disorder
- 50. Eric A. Storcha,b,⁎, Monica S. Wua,c, Brent J. Smalld, Erika A. Crawforda, Adam B. Lewina,b, Betty Hornga, Tanya K. Murphya,b aDepartment of Pediatrics, University of South Florida, St. Petersburg, FL 33701, USA bDepartment of Psychiatry and Behavioral Neurosciences, University of South Florida, St. Petersburg, FL 33701, USA cDepartment of Psychology, University of South Florida, St. Petersburg, FL 33701, USA dSchool of Aging Studies, University of South Florida, St. Petersburg, FL 33701, USA Abstract The current study examined correlates, moderators, and mediators of functional impairment in 98 treatment-seeking adults with obsessive–compulsive disorder (OCD). Participants completed or were administered measures assessing obsessive–compulsive symptom severity, functional impairment, resistance against symptoms, interference due to obsessive–compulsive symptoms, depressive symptoms, insight, and anxiety sensitivity. Results indicated that all factors, except insight into symptoms, were significantly correlated with functional impairment. The relationship between obsessive–compulsive symptom severity and functional impairment was not moderated by patient insight, resistance against obsessive–compulsive symptoms, or anxiety sensitivity. Mediational analyses indicated that obsessive–compulsive symptom severity mediated the relationship between anxiety sensitivity and obsessive–compulsive related impairment.
- 51. Indeed, anxiety sensitivity may play an important contributory role in exacerbating impairment through increases in obsessive– compulsive symptom severity. Depressive symptoms mediated the relationship between obsessive–compulsive symptom severity and obsessive–compulsive related impairment. Implications for assessment and treatment are discussed. © 2014 Elsevier Inc. All rights reserved. Obsessive–compulsive disorder (OCD) is a debilitating neuropsychiatric condition characterized by obsessions (i.e., recurrent and distressing thoughts, images, or impulses) and/ or compulsions (i.e., repetitive behaviors or mental acts performed to reduce distress) [1]. Although the severity of obsessive–compulsive symptoms is directly associated with the degree of functional impairment experienced [2–5], this relationship is not absolute; there are other variables that contribute to understanding who is at greater risk of compounded impairment and which mechanisms operate in influencing impairment. Accordingly, this study extends the literature by examining factors believed to be theoretically relevant in understanding impairment among treatment- seeking adults with OCD. ⁎ Corresponding author at: Department of Pediatrics, University of South Florida, 880 6th St. South, Box 460, St. Petersburg, FL 33701, USA. Tel.: +1 727 767 8230. E-mail address: [email protected] (E.A. Storch). 0010-440X/$ – see front matter © 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.comppsych.2013.10.014 To date, several studies have examined clinical charac-
- 52. teristics associated with functional impairment. In addition to obsessive–compulsive symptom severity, ability to resist and control obsessive–compulsive symptoms [2–4,6] and co-occurring depressive and anxiety symptoms [5–8] have been associated with functional impairment. Among children and adolescents with OCD, insight predicted parent- and child-rated functional impairment above and beyond obses- sive–compulsive symptom severity [19]. In an effort to understand potential mechanisms of impairment, one recent study of adults with OCD found that depressive symptoms and obsessive–compulsive symptom resistance/control me- diated the relationship between obsessive–compulsive symptom severity and functional impairment [6]. Although informative, other variables may be relevant in understand- ing why some individuals experience compounded impair- ment beyond that which is conferred by the degree of obsessive–compulsive symptom severity. Anxiety sensitivity has emerged as an important variable in understanding the development and maintenance of various http://www.sciencedirect.com/science/journal/0010440X http://www.sciencedirect.com/science/journal/0010440X http://dx.doi.org/10.1016/j.comppsych.2013.10.014 http://dx.doi.org/10.1016/j.comppsych.2013.10.014 http://dx.doi.org/10.1016/j.comppsych.2013.10.014 mailto:[email protected] http://dx.doi.org/10.1016/j.comppsych.2013.10.014 490 E.A. Storch et al. / Comprehensive Psychiatry 55 (2014) 489–496 anxiety disorders [9]. Defined as a fear of arousal- or anxiety- related sensations which are misinterpreted by the individual as harmful or dangerous [10], elevated anxiety sensitivity is associated with difficulty experiencing and tolerating anxiety-
- 53. related sensations [9]. Conceptually, anxiety sensitivity may relate to impairment by virtue of how someone with OCD experiences his or her symptoms and associated distress. An individual with high anxiety sensitivity may experience the distress associated with his or her obsessive–compulsive symptoms as unbearable and be more likely to engage in rituals or active avoidance of anxiogenic triggers, thus compounding impairment. Problematically, such behaviors contribute to the increased potential for illness chronicity through negative reinforcement (i.e., distress reduction) of obsessive–compulsive symptoms. A modest literature exists examining anxiety sensitivity among adults with OCD. Anxiety sensitivity levels were elevated in adults with OCD relative to non-clinical controls [11–13], and were at comparable levels to adults with non- OCD anxiety disorders [11]. There are a limited number of examinations into the association between anxiety sensitivity and obsessive–compulsive symptom severity. In 280 adults with OCD, Calamari et al. [14] found that anxiety sensitivity and obsessive–compulsive symptom severity were signifi- cantly related. Wheaton et al. [15] demonstrated modest associations between anxiety sensitivity and dimensional ratings of obsessive–compulsive symptoms in a large non- clinical sample of university students. Collectively, these studies suggest that OCD caseness is linked to elevated anxiety sensitivity relative to non-clinical samples, and may be directly linked with obsessive–compulsive symptom severity. However, these studies do not address the manner in which anxiety sensitivity may contribute to functional impairment, which has potential implications for the conceptualization and care of individuals with OCD. First, anxiety sensitivity may be one method through which obsessive–compulsive symptom severity is exacerbated and/or maintained. As stated, high anxiety severity may be linked to greater ritualizing/avoidance and less symptom
- 54. resistance, contributing to impairment and sustained symp- tomology. Second, anxiety sensitivity may be linked to a more chronic symptom course. Individuals with high anxiety sensitivity may be less likely to exhibit decreases in symptom severity relative to those with lower anxiety sensitivity [16], perhaps explaining, in part, the chronic nature of OCD in the absence of treatment. Beyond anxiety sensitivity, other variables may hold relevance in understanding which individuals may experi- ence compounded impairment. Insight into the degree to which obsessive–compulsive symptoms are recognized by the person as absurd, excessive, and senseless has been linked to obsessive–compulsive symptom severity and functional impairment in past studies of adults [17] and children with OCD [18,19]. Additionally, individuals with poor insight into their OCD symptomology have exhibited more complicated clinical presentations and poorer treatment response when compared to individuals with higher insight [17,20]. It is reasonable to consider that insight may moderate the relationship between obsessive–compulsive symptom severity and impairment such that those with poor insight may be more clinically complex and be less able to function effectively or actively challenge symptoms. Simi- larly, symptom resistance is also hypothesized to be relevant in understanding who is at risk for greater impairment in that those who actively try to challenge their symptoms would be less likely to experience OCD-related impairment. Indeed, the lower levels of resistance against obsessive–compulsive symptoms have been linked with increased obsessive– compulsive symptom severity [21], as well as decreased functioning and higher impairment [6,22]. In the present study, we examine correlates, moderators, and mediators of functional impairment in adults with OCD. Our specific study questions and hypotheses were as
- 55. follows. First, what are the relations among domains of functional impairment and obsessive–compulsive symptom severity, symptom resistance, interference due to obsessive– compulsive symptoms, anxiety sensitivity, depressive symptoms, and insight? We expected that the varied domains of functional impairment would be directly associated with obsessive–compulsive symptom severity, interference due to obsessive–compulsive symptoms, anx- iety sensitivity, and depressive symptoms, and inversely related to symptom resistance and insight. Second, we examined the extent to which insight, resistance against obsessive–compulsive symptoms, and anxiety sensitivity moderated the relationship between obsessive–compulsive symptom severity and OCD-related impairment. We expected that each variable would moderate this association such that the relationship between obsessive–compulsive symptom severity and OCD-related impairment would be more robust for those with lower insight and symptom resistance, and higher anxiety sensitivity. Third, would the relationship between anxiety sensitivity and OCD-related functional impairment be mediated by obsessive–compul- sive symptom severity? We predicted that as anxiety sensitivity increased, obsessive–compulsive symptom se- verity would increase, which would be positively associated with functional impairment. Finally, in an effort to replicate Storch et al. (2009), would the relationship between obsessive–compulsive symptom severity and OCD-related functional impairment be mediated by depressive symp- toms? We expected that as obsessive–compulsive symptom severity increased, depressive symptoms would increase, which would be directly associated with augmented functional impairment. 1. Method 1.1. Participants and procedures
- 56. Participants included 98 adults with a primary diagnosis of OCD that presented to an OCD specialty center to initiate 491E.A. Storch et al. / Comprehensive Psychiatry 55 (2014) 489–496 cognitive–behavioral treatment (Table 1). Diagnoses were established using best estimate diagnostic procedures in which consensus between two experienced clinicians (one of whom interviewed the participant in an unstructured assessment) was required on the primary diagnosis and the presence of comorbid diagnoses. Clinicians used all available information to ascertain an accurate diagnostic profile by including clinical information gleaned from an unstructured clinical interview, reviewing participants’ completed measures as part of this study, and examining past clinical records. Participants were excluded in the absence of 100% agreement for the primary or comorbid diagnoses, or if diagnosed with psychosis, mental retarda- tion, or bipolar disorder. The participants were between 18 and 72 years of age (M = 33.1, SD = 13.53) and were 57% female. The sample was 84% Caucasian, 10% Hispanic, 2% African American, 2% Asian, and 2% classified as ‘other.’ Common comorbid diagnoses included depression (57%), generalized anxiety disorder (30%), impulse control disorder-not otherwise specified (12%), and social phobia (10%). Seventy-nine participants (81%) reported currently taking psychotropic medication. All study procedures were approved by the local institutional review board. Following a regularly scheduled clinic visit, patients appropriate for the study were approached by a member of the research team who was otherwise uninvolved in the individual’s care to review the study; interested participants provided their written consent.
- 57. Participants then were administered the Yale–Brown Obsessive Compulsive Scale (Y-BOCS) [23,24] by a trained rater and thereafter completed self-report measures. Based on the Y-BOCS interview, the clinician rated the National Institutes of Mental Health Global Obsessive Compulsive Table 1 Demographic characteristics of the study sample (n = 98). Variable Gender (Male/Female) 41 Males (42%)/57 Females (58%) Age (Years) M = 33.10, SD = 13.53 Range = 18 to 72 years Race/Ethnicity Caucasian n = 82 (84%) Hispanic n = 10 (10%) African–American n = 2 (2%) Asian n = 2 (2%) Other n = 2 (2%) Comorbid Diagnosesa Depressive disordersb n = 56 (57%) Generalized anxiety disorder n = 29 (30%) Impulse control disorder not otherwise specified n = 12 (12%) Social phobia n = 10 (10%) Taking Psychotropic Medication n = 79 (81%) a The four most common comorbidities are listed in the table. Comorbid diagnoses occurring with less frequency are not reported.
- 58. b Depressive disorders included those diagnosed with major depression, dysthymia, and depressive disorder not otherwise specified. Scale (NIMH-GOCS) [25]. All independent evaluators underwent extensive training with the first author in the administration of Y-BOCS and NIMH-GOCS. 1.2. Measures 1.2.1. Yale–Brown Obsessive Compulsive Scale (Y-BOCS) [23,24] The Y-BOCS is a clinician-administered semi-struc- tured interview that assesses the presence and severity of obsessive–compulsive symptoms. Insight into obsessive– compulsive symptoms (item #11 on the Y-BOCS; possible score ranges from 0 to 4), interference due to obsessive–compulsive symptoms (sum of items #1, 2, 3, 6, 7, and 8; possible scores ranging from 0 to 24), resistance against obsessive–compulsive symptoms (sum of items #4, 5, 9, and 10; possible scores ranging from 0 to 16), and Severity Scale total score (possible scores ranging from 0 to 40) were all gathered through this measure. Higher scores on insight indicate poorer insight, higher scores on interference indicate higher interference, and higher scores on resistance indicate greater difficulty with resistance. The Y-BOCS has demonstrated excellent psychometric properties with regard to reliability and validity [26–28]. 1.2.2. Sheehan Disability Scale (SDS) [29] The SDS is a 3-item self-report questionnaire that assesses the level of impairment experienced due to obsessive–compulsive symptoms in social, occupational, and family life. The impairment scores for each domain
- 59. (possible scores range from 0 to 10) and the total score were used (possible scores range from 0 to 30), and higher scores indicate higher impairment. The SDS has shown good psychometric properties with regard to internal consistency and validity [30,31]. 1.2.3. National Institutes of Mental Health Global Obsessive Compulsive Scale (NIMH-GOCS) [25] The NIMH-GOCS is a one-item clinician-administered measure that assesses the severity of obsessive–compulsive symptoms on a scale from 1 to 15, with higher scores indicating more severe obsessive–compulsive symptoms. 1.2.4. Beck Depression Inventory-Second Edition (BDI-II) [32] The BDI-II is a 21-item self-report questionnaire that assesses the presence and severity of depressive symptoms in the past week. The total score was used (possible scores range from 0 to 63), and higher scores on the BDI-II indicate more depressive symptoms. The BDI-II has demonstrated adequate validity and reliability, including discriminant and construct validity, internal consistency, and test-retest reliability [32,33]. 1.2.5. Anxiety Sensitivity Index-Revised (ASI-R) [34] The ASI-R is a 36-item self-report questionnaire that assesses the respondent’s fear of anxiety and its respective sensations, due to the perceived negative consequences of Table 2 Correlation coefficients, means, standard deviations, and ranges for all study measures (n = 98).
- 60. 1 2 3 4 5 6 7 8 9 10 11 1. SDS Total Score 0.79⁎⁎⁎ 0.88⁎⁎⁎ 0.83⁎⁎⁎ 0.65⁎⁎⁎ 0.17 0.76⁎⁎⁎ 0.31⁎⁎ 0.70⁎⁎⁎ 0.72⁎⁎⁎ 0.26⁎ 2. SDS Work 0.55⁎⁎⁎ 0.45⁎⁎⁎ 0.57⁎⁎⁎ 0.11 0.65⁎⁎⁎ 0.22⁎ 0.58⁎⁎⁎ 0.54⁎⁎⁎ 0.14 3. SDS Social 0.65⁎⁎⁎ 0.56⁎⁎⁎ 0.19 0.64⁎⁎⁎ 0.33⁎⁎ 0.62⁎⁎⁎ 0.68⁎⁎⁎ 0.30⁎⁎ 4. SDS Family/Home 0.51⁎⁎⁎ 0.13 0.62⁎⁎⁎ 0.23⁎ 0.56⁎⁎⁎ 0.58⁎⁎⁎ 0.20⁎ 5. NIMH GOCSa 0.21⁎ 0.86⁎⁎⁎ 0.47⁎⁎⁎ 0.84⁎⁎⁎ 0.51⁎⁎⁎ 0.26⁎ 6. Y-BOCS Insight 0.17 0.31⁎⁎ 0.27⁎⁎ 0.22⁎ 0.08 7. Y-BOCS Interference 0.38⁎⁎⁎ 0.90⁎⁎⁎ 0.59⁎⁎⁎ 0.30⁎⁎ 8. Y-BOCS Resistance 0.74⁎⁎⁎ 0.30⁎⁎ 0.18 9. Y-BOCS Total Score 0.57⁎⁎⁎ 0.30⁎⁎ 10. BDI-II Total Scorea 0.37⁎⁎⁎ 11. ASI-R Total Scorea Mean 19.26 6.27 6.36 6.63 9.26 0.62 15.00 9.44 24.44 21.93 47.45 SD 7.16 2.79 3.01 2.76 2.10 0.86 3.73 2.35 5.10 11.31 28.91 Range 0–30 0–10 0–10 0–10 5–13 0–3 7–24 4–16 13–36 0–49 0–122 ⁎ p b 0.05. ⁎⁎ p b 0.01. ⁎⁎⁎ p b 0.001. a Indicates sporadic missing data. NIMH GOCS (n = 95), BDI-II
- 61. (n = 97), ASI-R (n = 97). 492 E.A. Storch et al. / Comprehensive Psychiatry 55 (2014) 489–496 the feelings. The total score was used (possible scores range from 0 to 144), with higher scores indicating greater anxiety sensitivity. The ASI-R has been shown to be psychometri- cally sound as demonstrated through high internal consis- tency and reliability [35]. The ASI-R also contains six factorially derived subscales, investigating: (1) fear of cardiovascular symptoms, (2) fear of respiratory symptoms, (3) fear of gastrointestinal symptoms, (4) fear of publicly observable anxiety reactions, (5) fear of dissociative and neurological symptoms, and (6) fear of cognitive dyscontrol. 1.3. Statistical analyses Prior to analysis, variables were evaluated for the presence of outliers and multicollinearity, and distributional properties were examined. For the moderation effects in regression, analyses were conducted using the MODPROBE macro through SPSS as described by Hayes and Matthes [36]. The mediation analyses were computed in Mplus [37] with bootstrapped standard errors for the direct and indirect effects. This method provides the same basic information as the classic Baron and Kenny [38] approach, but provides a specific test for the mediated effect and increases statistical power through the bootstrapped resampling [39]. For the correlations, there were sporadic missing values and the pairwise sample sizes are reported. For the moderation and mediation analyses, multiple imputation using SAS Proc MI [40,41] and maximum likelihood estimates using Mplus were employed, respectively. 2. Results 2.1. Descriptive statistics and correlations
- 62. Descriptive statistics (i.e., mean, standard deviation, and range) were calculated for all study variables (see Table 2). Pearson correlation coefficients were calculated for all study variables and statistical significance was adjusted for multiple comparisons using the Holm- Bonferroni correction [42]. Regardless of examining corrected or non-corrected correlations, all variables remained significantly correlated with the SDS total score (OCD-related impairment), except for insight into obses- sive–compulsive symptoms. Specifically, the SDS total score demonstrated a strong positive correlation with obsessive–compulsive symptom severity (NIMH GOCS, Y-BOCS Total score), interference (Y- BOCS Interfer- ence), and depressive symptoms (BDI-II), a moderate positive correlation with resistance against obsessive– compulsive symptoms (Y-BOCS Resistance), and a weak positive correlation with anxiety sensitivity (ASI-R). Impairment in work possessed a strong positive correlation with obsessive–compulsive symptom severity, interference, and depressive symptoms, and a weak positive correlation with resistance against obsessive–compulsive symptoms and anxiety sensitivity. Social impairment exhibited a strong positive correlation with obsessive–compulsive symptom severity, interference, and depressive symptoms, and a moderate positive correlation with resistance against obsessive–compulsive symptoms and anxiety sensitivity. Lastly, impairment in family life or home responsibilities demonstrated a strong positive correlation with obsessive–compulsive symptom severity, interference, and depressive symptoms, and a weak positive correlation with resistance against obsessive–compulsive symptoms and anxiety sensitivity. No impairment domain possessed a statistically significant correlation with insight into obsessive–compulsive symptoms.
- 63. To explore potentially differential relationships between specific components of anxiety sensitivity and obsessive– compulsive symptom severity, Pearson correlation coeffi- cients were also run to examine the relationship between 493E.A. Storch et al. / Comprehensive Psychiatry 55 (2014) 489–496 each subscale on the ASI-R and the Y-BOCS Total score (Table 3).1 Fear of cardiovascular symptoms (subscale 1) and fear of gastrointestinal symptoms (subscale 3) did not demonstrate statistically significant correlations with obsessive–compulsive symptom severity. Fear of respiratory symptoms (subscale 2), fear of publicly observable anxiety reactions (subscale 4), fear of dissociative and neurological symptoms (subscale 5), and fear of cognitive dyscontrol (subscale 6) all shared weak to moderate relationships with obsessive–compulsive symptom severity. 2.2. Moderation analyses Insight into obsessive–compulsive symptoms, resistance against obsessive–compulsive symptoms, and anxiety sen- sitivity were not significant moderators of the relationship between obsessive–compulsive symptom severity and OCD-related impairment. In testing insight, resistance, and anxiety sensitivity as potential moderators, NIMH GOCS was a significant predictor of OCD-related impairment (β = 2.04, p b 0.0001; β = 2.05, p b 0.0001; β = 1.89, p b 0.0001), respectively. However, insight was not a significant predictor of OCD-related impairment (β = 0.60, p = 0.40), and neither was the interaction term for NIMH GOCS and insight (β = −0.31, p = 0.41). Additionally, neither resistance (β = 0.05, p = 0.87) nor the interaction term between NIMH GOCS and resistance was a significant
- 64. predictor for OCD-related impairment (β = −0.20, p = 0.09). Lastly, anxiety sensitivity was not a significant predictor of OCD-related impairment (β = 0.04, p = 0.09), nor was the interaction term between NIMH GOCS and anxiety sensitivity (β = −0.01, p = 0.17). 2.3. Mediation analyses2 Obsessive–compulsive symptom severity (NIMH GOCS) was tested as a potential mediator between anxiety sensitivity (ASI-R) and OCD-related impairment (SDS). The indirect effect was statistically significant (β = 0.03, SE = 0.01, p b 0.05) suggesting that the relationship between anxiety sensitivity and OCD-related impairment was explained by symptom severity, with higher anxiety sensitivity scores associated with higher obsessive– compulsive symptom severity scores (β = 0.02, SE = 0.01, p b 0.05), and higher obsessive–compulsive symptom severity scores associated with higher OCD-related impair- ment (β = 2.11, SE = 0.26, p b 0.001). Finally, the direct effect between anxiety sensitivity and OCD-related impair- 1 Correlations with each ASI-R subscale remained statistically significant with highly comparable strengths when the correlations were re-run with NIMH GOCS as the measure of OCD symptom severity. 2 All mediating effects remained the same when the mediation analyses were re-run with Y-BOCS Total score as the measure of OCD symptom severity. As such, NIMH GOCS was utilized as the metric for OCD symptom severity throughout the moderation and mediation analyses to maintain consistency.
- 65. ment was no longer statistically significant after the mediator was added to the model (β = 0.03, SE = 0.02, p = 0.17). Depressive symptoms were tested as a potential mediator between obsessive–compulsive symptom severity (NIMH GOCS) and OCD-related impairment (SDS). The results demonstrated that depressive symptoms were a statistically significant mediator, with an indirect effect of 0.94 (SE = 0.19, p b 0.001) suggesting that the relationship between symptom severity and OCD-related impairment was explained by depressive symptoms, with higher scores on obsessive–compulsive symptom severity associated with higher depressive symptoms (β = 2.81, SE = 0.43, p b 0.001), and higher scores on depressive symptoms being associated with higher OCD-related impairment (β = 0.33, SE = 0.05, p b 0.001). Although the indirect effect was statistically significant, the direct effect of obsessive– compulsive symptom severity and OCD-related impairment was also statistically significant (β = 1.26, SE = 0.27, p b 0.001). 3. Discussion We report on correlates, moderators, and mediators of functional impairment in adults with OCD. As expected, domains of impairment were strongly related to obsessive– compulsive symptom severity and interference, and mod- estly associated with symptom resistance and depressive symptoms. Relations of this magnitude are reflective of the impairing and distressing nature associated with obsessive– compulsive symptom severity. Indeed, OCD distinguishes itself from other anxiety disorders in terms of the degree of impairment [43], which contributes to it being listed as a leading cause of disability [44,45]. Weak associations were found between impairment and anxiety sensitivity and insight, which suggest that OCD caseness confers greater risk for impairment regardless of insight or anxiety
- 66. sensitivity, such that more severe presentations are not necessarily linked with limited insight. It may also be that those with poor insight have similarly limited awareness into their own impairment. Additionally, only certain subscales on the assay of anxiety sensitivity were significantly correlated with obsessive–compulsive symptom severity, which may suggest that fear of cardiovascular and gastrointestinal symptoms may be less related to obses- sive–compulsive symptom severity when compared to other domains of anxiety sensitivity. Furthermore, the strength of the statistically significant correlations with obsessive– compulsive symptom severity was highly comparable not only across the ASI-R subscales, but also with the ASI-R total score. As such, it appears that the fears of respiratory symptoms, publicly observable anxiety reactions, dissocia- tive and neurological symptoms, and cognitive dyscontrol do not seem to show differential associations with obsessive– compulsive symptom severity when compared to one another, nor when compared to anxiety sensitivity as a Table 3 Correlation coefficients, means, standard deviations, and ranges for ASI-R subscales and OCD symptom severity (n = 98). 1 2 3 4 5 6 7 1. Y-BOCS Total Score 0.13 0.29⁎⁎ 0.12 0.29⁎⁎ 0.27⁎⁎ 0.28⁎⁎ 2. ASI-R S1: Fear of Cardiovascular Symptomsa 0.59⁎⁎⁎ 0.59⁎⁎⁎ 0.45⁎⁎⁎ 0.69⁎⁎⁎ 0.36⁎⁎⁎ 3. ASI-R S2: Fear of Respiratory Symptoms 0.43⁎⁎⁎ 0.53⁎⁎⁎ 0.75⁎⁎⁎ 0.46⁎⁎⁎
- 67. 4. ASI-R S3: Fear of Gastrointestinal Symptomsa 0.43⁎⁎⁎ 0.64⁎⁎⁎ 0.20⁎ 5. ASI-R S4: Fear of Publicly Observable Anxiety Symptoms 0.64⁎⁎⁎ 0.48⁎⁎⁎ 6. ASI-R S5: Fear of Dissociative and Neurological Symptomsa 0.65⁎⁎⁎ 7. ASI-R S6: Fear of Cognitive Dyscontrola Mean 24.44 6.57 9.10 3.32 14.40 7.89 6.32 SD 5.10 6.18 7.77 4.19 7.28 5.58 5.94 Range 13–36 0–23 0–28 0–16 0–32 0–23 0–20 ⁎ p b 0.05. ⁎⁎ p b 0.01. ⁎⁎⁎ p b 0.001. a Indicates sporadic missing data. ASI-R Subscales 1, 3, 5, and 6 (n = 97). 494 E.A. Storch et al. / Comprehensive Psychiatry 55 (2014) 489–496 construct in general. These results suggest that relatively equal consideration should be given to the respective components of anxiety sensitivity when considering their relationship with OCD symptom severity. One of the primary findings of interest was that obsessive–compulsive symptom severity mediated the relationship between anxiety sensitivity and OCD-related impairment. Stated differently, as anxiety sensitivity in- creased, obsessive–compulsive symptom severity increased, which was directly associated with augmented functional impairment. This is consistent with past findings implicating the role of anxiety sensitivity and symptom severity [14,16],
- 68. and provides a potential mechanism through which anxiety sensitivity exacerbates symptom severity and ultimately functional impairment. Among individuals presenting with elevated anxiety sensitivity, this may trigger more severe clinical presentations characterized by extreme distress, decreased distress tolerance, and difficulty resisting/control- ling obsessive–compulsive symptoms, which translate into greater functional impairment relative to those with lower levels of anxiety sensitivity. Speculatively, anxiety sensitiv- ity may be one variable associated with attenuated homework compliance in exposure and response prevention treatment. That is, individuals with high anxiety sensitivity may be less likely to independently engage in homework tasks as they may find the experience too distressing. Problematically, homework compliance is a key element of psychotherapeutic treatment in which poor compliance is associated with reduced response [46,47]. Similar to past findings [6], the relationship between obsessive–compulsive symptom severity and OCD-related functional impairment was mediated by depressive symp- toms, such that as obsessive–compulsive symptom severity increased, depressive symptoms correspondingly increased, contributing to greater functional impairment. Studies document the temporal association between obsessive– compulsive symptom onset and a corresponding increase in depressive symptoms [48], which is believed to be secondary to the distressing and time intensive nature of obsessive–compulsive symptoms. The contribution of depressive symptoms to the clinical picture of OCD may increase risk for impairment by virtue of additional psychiatric morbidity or the interactional nature of having two impairing problems. Correspondingly, there is evidence that reducing obsessive–compulsive symptoms through evidence-based OCD interventions translates into improve- ments in depressive symptomology [49,50]. Thus, treating
- 69. obsessive–compulsive symptoms may be one method of improving comorbid depressive symptoms that are function- ally related to OCD. However, this approach may not translate to all patients; modular interventions that are personalized to individual patient characteristics such as comorbid depression would be well-suited for this cohort. Interestingly, insight into obsessive–compulsive symp- toms, resistance against obsessive–compulsive symptoms, and anxiety sensitivity did not significantly moderate the relationship between obsessive–compulsive symptom se- verity and OCD-related functional impairment. Regarding insight, past studies, including this one, have found relatively weak associations between symptom insight and obsessive– compulsive symptom severity [51–53]. This suggests that insight may not be the driving force in understanding why some people are more impaired than others. It may be that people with very limited insight are not aware of the degree to which they are impacted by their symptoms; alternatively, they may have family members who are providing significant accommodation with the goal of reducing functional impairment. However, the finding that insight was not a significant mediator may also be attributed to a range restriction problem with the variable; upon examina- tion of the mean and standard deviation for the insight variable within this sample, a truncated range was indeed observed and could have been the source of precluding support for the hypothesis. It is somewhat surprising that resistance against obsessive–compulsive symptoms did not moderate the association between symptom severity and impairment, as it was expected that those who resist less would be more likely to experience impairment as their 495E.A. Storch et al. / Comprehensive Psychiatry 55 (2014)
- 70. 489–496 symptoms increased. Although there are clearly merits of resisting symptoms, it may be that symptom resistance yields differential effects across people; that is, some people may experience some cathartic benefits associated with reduced impairment, while others may not experience the same benefits through the emotional and tangible efforts required for successful resistance. It may be that anxiety sensitivity does not function as a moderator but rather exerts its effect through mediation by contributing to obsessive–compulsive severity, which in turn compounds functional impairment. Several limitations to this study should be noted. First, the generalizability of the results may be restricted due to demographics of the study sample, as participants were primarily Caucasian and seeking treatment for their OCD. Second, the study was cross-sectional, limiting the ability to establish causality. Third, our assessment of insight relied on one clinician administered item and may not be as sensitive and/or comprehensive as using a tailored measure of insight (e.g., BrownAssessment ofBeliefs) or other related constructs, such as overvalued ideas (e.g., Overvalued Ideas Scale). Lastly, other variables not examined in the present study (e.g., cognitive variables) may be relevant in understanding the relationship between obsessive–compulsive symptoms and OCD-related impairment. Within these limitations, this study has important implica- tions for the care of individuals with OCD. First, these data speak to the importance of assessing anxiety sensitivity in addition to more traditional constructs (e.g., comorbidity, insight, etc.). Given that anxiety sensitivity is linked to elevated obsessive–compulsive symptom severity, which in turn is associated with increased functional impairment, evaluating the patient’s level of anxiety sensitivity may help identify potential risk factors for OCD-related impairment. Addressing
- 71. heightened anxiety sensitivity in treatment may also help with improved tolerability and quicker habituation to anxiety- producing situations, aiding in the process of exposure and response prevention. However, it remains unclear if anxiety sensitivity improves through standard therapies (e.g., cognitive behavioral therapy, antidepressant medications) or requires alternative, adjunctive approaches (e.g., interoceptive expo- sure) [54]. Second, depressive symptoms should correspond- ingly be assessed; these symptoms may serve as an underlying mechanism that is influenced by obsessive–compulsive symptom severity, ultimately contributing to functional impairment. As such, it is important to monitor the severity of depressive symptoms as treatment progresses, examining any changes (or lack thereof) secondary to the alleviation of obsessive–compulsive symptoms. Given the influence of depressive symptomology on functional impairment, any substantial symptoms remaining after OCD treatment may warrant more targeted interventions for the depression. Collectively, it is important to consider variables that contribute to OCD-related disability, as it allows clinicians to better predict risk factors and utilize targeted interventions to decrease functional impairment. Given the association with decreased functioning and poorer treatment response [55], prudent identification and interventions for these constructs are hoped to help improve the prognosis of individuals with OCD. References [1] American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013. [2] Bystritsky A, Liberman RP, Hwang S, Wallace CJ, Vapnik T,
- 72. Maindment K, et al. Social functioning and quality of life comparisons between obsessive–compulsive and schizophrenic disorders. Depress Anxiety 2001;14(4):214-8. [3] Bobes J, Gonzalez MP, BascaranMT, Arango C, Saiz PA, BousonoM. Quality of life and disability in patients with obsessive– compulsive disorder. Eur Psychiatry 2001;16(4):239-45. [4] GrabeHJ,Meyer C,HapkeU, RumpfHJ, Freyberger HJ, Dilling H, et al. Prevalence, quality of life and psychosocial function in obsessive– compulsive disorder and subclinical obsessive–compulsive disorder in Northern Germany. Eur Arch Psychiatry Clin Neurosci 2000;250(5): 262-8. [5] Huppert JD, Simpson HB, Nissenson KJ, Liebowitz MR, Foa EB. Quality of life and functional impairment in obsessive– compulsive disorder: a comparison of patients with and without comorbidity, patients in remission, and healthy controls. Depress Anxiety 2009; 26(1):39-45. [6] Storch EA, Abramowitz JS, Keeley M. Correlates and mediators of functional disability in obsessive–compulsive disorder. Depress Anxiety