
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Clinic based management of vertigo.
Similar to Clinic based management of vertigo. (20)
More from Prasanna Datta
More from Prasanna Datta (20)
Recently uploaded
Recently uploaded (20)
Clinic based management of vertigo.
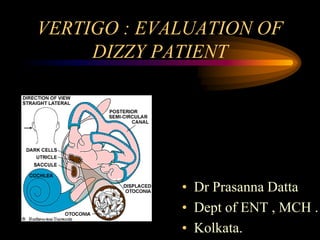
- 1. VERTIGO : EVALUATION OF DIZZY PATIENT • Dr Prasanna Datta • Dept of ENT , MCH . • Kolkata.
- 2. INTRODUCTION • Vertigo is the illusion of motion, usually rotational motion • The word dizzy includes a broad range of sensations from severe vertigo to momentary light headedness. • Light headedness is pre syncopal rather than vestibular in origin.( Non vestibular form of dizziness)
- 3. INCIDENCE OF DISEASE • About 30-35% of the population experience episodes of vertigo by the age of 65 years. • It is a common complaint in clinical practice, seen in about 10-15% of patients seen by an Otorhinolaryngologist • Diagnosis of the condition remains a challenge for the family physician as well as among otolaryngologists.
- 4. MANAGEMENT • Good management depends upon an accurate diagnosis. • Initial approach to evaluate the dizzy patient is to consider the categories of dizziness in the the differential diagnosis. • To determine whether the dizziness is vestibular or non vestibular in origin
- 5. VESTIBULAR ORIGIN Peripherial One ear involved or both ear involved Central Brain stem or brain
- 6. • A proper history and a detailed clinical examination is followed by appropriate investigations to come to a correct diagnosis. • History of illness as emergent acute & chronic helps to clinch the tentative underlying cause of vertigo. Acute dizziness - CNS hemorrhages and infarcts need immediate intervention. Trauma to inner ear or temporal bone and bacterial labyrinthitis require urgent treatment.
- 7. DIFFERENTIAL DIAGNOSIS FOR VERTIGO Vestibular disorders that cause Vertigo Peripheral Central Meniere’s disease VBI BPPV PICAS Vestibular neuronitis Basilar migraine Labyrinthitis Cerebellar disease Vestibulotoxic drugs Multiple sclerosis Head trauma Tumours of brainstem Perilymph fistula Epilespy Syphilis Cervical vertigo Acoustic neuroma
- 10. DURATION SPELL Seconds BPPV,labyrinthine fistula Cervical vertigo,VBI Minutes TIA Hours meneier’s disease Days viral neuro labyrinthitis Variable migraine
- 11. HISTORY TAKING • Past H/O Head injury – Operation Fever • Personal H/O BP (high or low) Diabetes Alcohol, tobaco Otorrhea Heart disease Arthritis
- 12. CLINICAL EXAMINATION • General medical examination • Specific clinical exam. of vestibular pathology Otological examination – fistula test Vestibulo-ocular examination Eye movements Spontaneus nystagmus Positional nystagmus • Neuro otological examination Romberg test Tandem walking Eye open Eye closed Fukuddas stepping test positional nystagmus test DIX-HALLPIKE maneuver
- 13. • DIX HALLPIKE
- 15. INVESTIGATION • ENG:recording of eye movements that allows precise quantification of both physical and pathological nystagmus Sponatanous nystagmus Gaze nystagmus Pendulam tracking test Caloric test • CCG-photo graphic recording of patient’s head and body movements Functional measurement of balance that reflexes vestibulospinal function
- 16. • Rotatory test- Barany’s technique- nystagmus induced by sudden stop is 10 to 30 sec in duration in normal subject.which is fairly symmetrical in clock wise and counter clock wise in rotation.Gross asymmetries in the duration between the responses to clockwise and counter clockwise rotation are taken as a vestibular pathology. • By ENG pre rotatory as well as post rotatory nystagmus is evaluated
- 17. PTA SRT SDS Tone decay • BERA –method of plotting electrical activities in response to auditory or vestibular stimuli. • Caloric test – kobrak’s cold caloric test a)(2 to 5cc of ice cold water) to initiate vertigo with labyrinthine type of nystagmus b)10 to 20 cc of ice cold water initiate nystagmus-canal paresis c) No nystagmus or vertigo after 40 cc of ice cold water –dead . labyrinthine AUDIOMETRIC TEST
- 18. IMAGING • Conventional Xrays Xray mastoids , laws lateral view Xray skull per orbital view X ray PNS, water’s view Xray cervical spine AP, lateral view • MRI &MRI angiographic study • CT / CT angiographic study • EEG • EMG • NCV
- 19. HAEMATOLOGICAL STUDY • Routine blood test :Hb%,TLC,DLC,blood for sugar (F) & PP, serum cholesterol, serum triglyceride. • Serological test for syphilis • Thyroid function test
- 23. VESTIBULAR DISORDERS DIAGNOSTIC CONSEPT AND ALGORITHMS • Benign paroxysmal positional vertigo (BPPV) • Vestibular neuritis • Benign paroxysmal vertigo of childhood • Motion sickness • Meniere’s disease / endolymphatic hydrops • Labyrinthine disease of metabolic origin • Autommune inner ear disease • Otoxicity • Vestibular schwannoma
- 24. PHYSICAL EXERCISE REGIMENS Habituation and adaptive response and sensory substitution Vestibular rehabilitation refers to a structural programme of treatment aimed at expediting and enhancing vestibular compensation and rendering dizzy patient ,asymptomatic such that they can return to full occupational and social activities. Systemic exercise programme eg. Cawthorne- cooksey exercises Specific therapies Epley maneuvere( canalolith repositioning method), Semont maneuvere
- 25. Cawthrone cooksey exercise EXERCISES IN BED : EYE MOVEMENTS Looking up and then down
- 26. EXERCISES IN BED : EYE MOVEMENTS Looking alternately left and right
- 28. EXERCISES IN BED : HEAD MOVEMENTS Bending alternately forward and backward
- 29. EXERCISES IN BED : HEAD MOVEMENTS Turning alternatively to the left and then right
- 30. EXERCISES IN SITTING POSITION Shrugging and rotating shoulders
- 31. EXERCISES IN SITTING POSITION Bending forward and picking up objects from the floor
- 32. EXERCISES IN SITTING POSITION Turning head and trunk alternately to the left and the right
- 33. EXERCISES IN STANDING POSITION Changing from sitting to standing, initially with eyes open and then with the eyes closed
- 34. Throwing a small (ping pong) ball in an arc from hand to hand and following it with the eyes
- 35. Throwing a small ball from hand to hand under the knee
- 36. EXERCISES WHILE WALKING Throwing and catching the ball while walking
- 37. EXERCISES WHILE WALKING Walking around in the room with eyes open and closed
- 38. EXERCISES WHILE WALKING Walking up and down a flight of stairs
- 39. EXERCISES WHILE WALKING Playing any game involving bending, stretching and aiming with the ball
- 40. OFFICE TREATMENT OF BPPV: The Epley maneuver •
- 41. from sitting position to ipsilateral lateral position. After 1 to 1.5 minute patient is moved 180 to the contralateral lateral position
- 42. INSTRUCTIONS FOR PATIENTS AFTER OFFICE TREATMENTS •
- 43. HOME TREATMENT OF BPPV Brandt –Daroff exercises
- 44. A Retrospective study in ENT dept, MCH. For Vestibular Exercises N = 48 patients (male 20, female 28) diagnosed as BPPV. Study period – Nov. 2005 – Nov 2006. Patients – randomly assigned to one of three groups. Follow up visit - 1 week, 2 weeks and 3 months.
- 45. Group 1 : Semont’s maneuver followed by post treatment (n = 16) instruction (sleep in sitting position for 2 nights plus then normal side for next 5 nights) Success rate : 75% (n = 12) after one treatment. Group 2 : Apley’s maneuver followed by post treatment (n = 16) instruction Success rate : 87.5% (n = 14) after one treatment Group 3 : Brandt-Daroff maneuver (repeated positioning (n = 16) exercises 3 times a day for 2 weeks) Success rate : 56.25% (n = 9) Overall success rate of vestibular rehabilitation exercises is73% (approx)
- 46. CONCLUSION Some important point to remember • Vertigo is a symptom not a disease. • In most vertigo underlying cause is simple • Art of history taking for correct diagnosis is essential. • Vestibular rehabilitation exercises help a lot to relieve vertigo.