2. therapy in the spine surgery setting.
METHODS: Researchers used a two-group randomized
control design to evaluate the effects of local cold therapy
on postoperative pain and analgesia use after lumbar spinal
fusion surgery. The primary outcome was postoperative
pain. Secondary outcomes included analgesia use and per-
ceived benefit of cold therapy.
RESULTS: The intervention (cold) group had a marginally
greater reduction in mean Numerical Rating Scale score
across all 12 pain checks (M ± SD = −1.1 ± 0.8 points
reduction vs. −1.0 ± 0.8 points reduction, p = .589). On
average, the intervention group used less morphine equiva-
lents (M ± SD = 12.6 ± 31.5 vs. 23.7 ± 40.0) than the
control group across pain checks seven to 12 (p = .042).
CONCLUSIONS: This study provides additional evidence to
support the use of cold therapy as an adjuvant pain man-
agement strategy to optimize pain control and reduce opi-
oid consumption following spine fusion surgical procedures.
Effects of Localized Cold Therapy on Pain
in Postoperative Spinal Fusion Patients
A Randomized Control Trial
Patricia Quinlan ▼ Jack Davis ▼ Kara Fields ▼ Pia Madamba
▼ Lisa Colman ▼
Daniela Tinca ▼ Regina Cannon Drake
Patricia Quinlan, PhD, MPA, RN, CPHQ, AVP Nursing
Excellence,
Department of Nursing, Hospital for Special Surgery, New
York, NY.
Jack Davis, MSN, RN, ONC, Manager, Patient Education
Programs and
Research, Department of Nursing, Hospital for Special Surgery,
New
3. York, NY.
Kara Fields, MS, Statistical Analyst, Healthcare Research
Institute,
Hospital for Special Surgery, New York, NY.
Pia Madamba, BSN, RN, ONC, Patient Care Director,
Department of
Nursing, Hospital for Special Surgery, New York, NY.
Lisa Colman, RN, ONC, Clinical Nurse, Department of Nursing,
Hospital
for Special Surgery, New York, NY.
Daniela Tinca, BSN, RN, ONC, Clinical Nurse, Department of
Nursing,
Hospital for Special Surgery, New York, NY.
Regina Cannon Drake, MA, RN, ONC, Patient Educator,
Department of
Nursing, Hospital for Special Surgery, New York, NY.
The authors have disclosed no conflicts of interest.
DOI: 10.1097/NOR.0000000000000382
et al., 2003; Konrath, Lock, & Goitz, 1996; Wahern,
Torebjork, & Jorum, 1989). Cold therapy is used in sports
and rehabilitation settings to treat tissue injuries and has
been found to be effective in reducing pain and swelling
after arthroscopy and arthroplasty surgery (Aide, Kwan,
Naylor, Harris, & Mittal, 2012; Bleakley, et al., 2004;
Kullenberg, Ylipaa, Soderlund, & Resch, 2006; Lessard,
Scudds, Amedola, & Vaz, 1997). Cold therapy with com-
pression has been shown to have additive benefits of re-
duced swelling, but findings from the studies also sug-
5. operative therapy with a cooling device used 49% less
patient-controlled analgesia (PCA) than the control
group patients who did not receive cold therapy
(Stephee, Booher, & Biscup, 1996). In addition, those
who received cold treatment reported an eight out of 10
satisfaction score with the intervention.
Findings across the limited number of studies using
cold therapies to manage the care of postoperative spine
patients suggest benefits to decreasing narcotic con-
sumption. Narcotics, specifically opiates, often require
additional care management strategies to address ad-
verse side effects including nausea, vomiting, constipa-
tion, sedation, dizziness and the potential for tolerance,
physical dependence, addiction, abuse, and diversion
(Benyamin et al., 2008).
The purpose of this study was to determine the ef-
fects of the application of cold (ice pack) on postopera-
tive spine pain fusion patients and add to the body of
knowledge specific to practical application in the spinal
fusion surgical setting. Given limited clinical evidence,
this study should inform practitioners on the benefits of
using cold therapy as an adjuvant therapy to reduce
pain and narcotic consumption in the management of
the postoperative spine patient population.
Methods
Design
Researchers used a two-group randomized control de-
sign to evaluate the effects of local cold therapy on post-
operative pain and analgesia use after lumbar spinal fu-
sion surgery. The primary outcome was postoperative
pain. Secondary outcomes included analgesia use and
perceived benefit of cold therapy. Participants were ran-
domly assigned to two strata: (a) lumbar spine fusion
6. patients with repositioning and application of cold ther-
apy and (b) lumbar spine fusion patients with reposi-
tioning and no application of cold therapy. Concealed
randomization schedule was generated by the biostatis-
tics department at the study organization, with rand-
omization lists provided to investigators after consent
and prior to treatment. Participants were assigned to
either the control or intervention group by the random
generator, and his/her treatment arm assignment was
placed in a concealed envelope. There was no blinding
of participants because it was obvious who received
cold therapy and who did not. The study was approved
by the organization’s institutional review board.
setting anD sample selection
Subjects were recruited from July 11, 2013, through
February 13, 2015, in their surgeons’ offices or the
preoperative holding center of an urban, acute care fa-
cility specializing in the treatment of musculoskeletal
diseases.
Participants were a convenience sample of adults
who underwent postoperative lumbar spinal fusion sur-
gery from one to four levels and were admitted to a spe-
cific inpatient surgical unit within 12 hours after sur-
gery. Preoperative inclusion criteria included (a) English
speaking and (b) 18 years or older. Exclusion criteria
included (a) non-English speaking, (b) intolerance to
cold, (c) medical history of rheumatoid arthritis, sclero-
derma, dermatological conditions, Reynaud’s phenom-
ena, and dementia, and (c) use of ice to lower back prior
to surgery.
Eligible participants were identified by the coinvesti-
gating surgeons who communicated to the principal in-
7. vestigator (PI), a nurse patient educator. The PI con-
tacted potential participants during the preoperative
scheduling process and served as the primary point per-
son to discuss study details and introduce the consent
form. The PI approached all identified potential partici-
pants before surgery. The consent was reviewed, outlin-
ing the approach and purpose of this study, which was
to determine whether cold therapy in the form of local
application of ice packs is effective in reducing postop-
erative pain in patients who have spine fusion surgery.
The concept of randomization was explained, inform-
ing subjects that they would be chosen by chance, to
give each participant an equal opportunity to be in-
cluded in the ice versus no-ice study group provided
they met study criteria postoperatively. Postoperative
exclusion criteria were as follows: prolonged stay in the
postanesthesia care unit, discharge to a nonstudy inpa-
tient unit, and surgical intervention that changed dur-
ing the operation.
Data on participant refusal were not collected for
analysis. Ninety-three participants who gave study con-
sent were not randomized to either intervention be-
cause of failure to meet postoperative criteria.
measurement
Pain levels were measured using the Numerical Rating
Scale (NRS). This is a valid and reliable measurement of
pain experienced by acute care patients (Hjermstad
et al., 2011; Wewers & Lowe, 1990). Participants ver-
bally reported a score from zero to 10, with zero repre-
senting no pain and 10 representing the worst pain im-
aginable. The NRS score was assessed both prior to and
following study interventions, coincided with the staff
protocol for routine 4-hour pain assessments and con-
tinued for every 4 hours until discharge. Pain checks
9. ice and applied to the lower back, and the pack was sup-
ported with a pillow. The cold packs were applied to the
intervention group and a timer was set for 20 minutes.
After 20 minutes the nurse removed the pack.
Participants were again asked to rate their pain level
using the NRS. Participants were also asked whether
the intervention reduced their pain.
Control Group
Procedures for the control group were the same as for
the intervention groups, with the exception of the cold
packs. During routine pain assessments, participants
were asked to rate their pain level using the NRS.
Participants were turned and positioned to a side-lying
position in bed. After 20 minutes, the nurse asked the
patient to rate his/her pain level using the NRS.
Participants were also asked whether the intervention
reduced their pain.
Nurses provided pain medication to all patients using
a standardized pain medication order set. Data were re-
corded every 4 hours and continued over a 48-hour pe-
riod for both groups.
Data analysis
It was determined that a sample size of 100 patients per
group would provide 98% power at a two-sided α level
of .05 for a two-sample t test to detect a two-point differ-
ence in NRS pain score change between groups (assum-
ing a within-group standard deviation of four points) at
24 and 48 hours postoperation. After an exploratory in-
terim analysis postrandomization of 70 patients, the
power analysis was revised. It was determined that a
sample size of 68 patients per group would provide 80%
power at a two-sided α level of .05 for a two-sample t test
to detect a two-point difference in NRS pain score
10. change between groups (assuming within-group stand-
ard deviation of four points) at 24 hours postoperation.
A total of 150 patients would be enrolled to account for
attrition.
The cold therapy and control groups were compared
for balance on baseline characteristics by calculating
standardized differences. Standardized differences
were calculated as the difference in means or mean
rankings divided by the pooled standard deviation for
normally distributed or ordinal variables and skewed
continuous variables, respectively (Austin, 2009;
Schacht, Bogaerts, Bluhmki, & Lesaffre, 2008). For cat-
egorical variables, standardized differences were calcu-
lated as the difference in proportions divided by the
pooled standard deviation (Austin, 2009). Imbalance
was defined as a standardized difference with an abso-
lute value greater than 21.96 0.322
74
=× (Austin, 2009).
Average change in the NRS pain score pre- to postin-
tervention and cumulative PCA usage across pain
checks one to six and seven to 12 were compared be-
tween groups after adjustment for preoperative pain
level using the generalized estimating equation (GEE)
method with an identity link (Ma, Mazumdar, &
Memtsoudis, 2012; Zeger, Liang & Albert, 1988). The
GEE method accounts for the correlation between re-
peated measurements on the same patient. Average
change in the NRS pain score pre- to postintervention
and cumulative PCA usage across pain checks one to 12
were compared between groups after adjustment for
preoperative pain level using linear regression. Patient
11. perception of intervention benefit was compared be-
tween groups after adjustment for preoperative pain
level using the GEE method with a logit link.
All statistical hypothesis tests were two-sided, with
p < .05 considered statistically significant. Statistical
analyses were performed with SAS Version 9.3 (SAS
Institute, Cary, North Carolina).
Results
stuDy participants
One hundred and forty-eight patients completed the
study. Participant characteristics are provided in Table 1.
Data comparisons demonstrate characteristic similarity
across groups. Data were reported on all completed pain
checks at each interval. Because of patient discharge,
withdrawal, or refusal, 63 patients in each group had
complete data for the sixth pain check. The lowest num-
ber of patients with complete data occurred during the
12th pain check with 53 and 61 patients in the cold ther-
apy and control groups, respectively.
nrs score
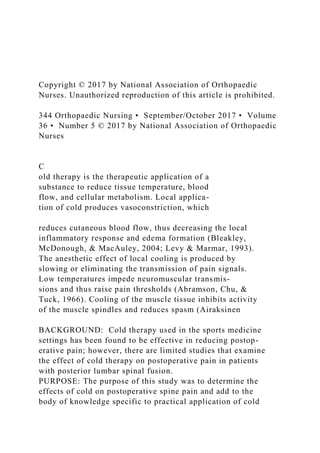
As summarized in Table 2 and Figure 1, our study
showed the intervention group had a marginally greater
reduction in mean NRS score across all 12 pain checks
(M ± SD = −1.1 ± 0.8 points reduction vs. −1.0 ± 0.8
points reduction, p = .589). The triangles represent the
means. The bottom and top of each rectangle indicate
the first and third quartiles, respectively. The horizon-
tal line within each rectangle indicates the median.
The lines extending out of the bottom and top of each
rectangle represent the minimum and maximum val-
ues that lie within 1.5 times the interquartile range
below and above the first and third quartiles, respec-
tively. The results demonstrate both groups had re-
13. Our finding of significant reduction in analgesia use
by the participants who received cold therapy is consist-
ent with results of two similar studies that measured
this outcome (Brander et al., 1996; Fountas et al., 1999).
Significance of this finding cannot be overstated, as opi-
oids are commonly used postoperatively by patients
table 1. participant characteristics
Control (n = 74) Cold Therapy (n = 74) Standardized Difference
Age, M ± SD 61.4 ± 14.9 62.4 ± 11.7 0.075
Female, n (%) 48 (64.9) 42 (56.8) −0.167
White, n (%) 64 (86.5) 66 (89.2) 0.083
Employment status, n (%)
Employed 42 (56.8) 44 (59.5) −0.047
Unemployed 5 (6.8) 8 (10.8) 0.121
Other 21 (28.4) 22 (29.7) −0.025
Unknown 6 (8.1) 0 (0) −0.420
Medical insurance, n (%)
Yes 70 (94.6) 74 (100) 0.239
Workman’s comp 2 (2.7) 0 (0) −0.239
Unknown 2 (2.7) 0 (0) −0.236
Duration of back pain, n (%) −0.174
16. size, a larger sample is always preferable. The study was
conducted on one inpatient unit at an orthopaedic sur-
gical specialty hospital; therefore, the results may not be
generalized to other institutions.
implications for practice anD research
The results demonstrate decreased analgesic consump-
tion and a trend in lower NRS pain scores in the inter-
vention group and a perceived reduction of pain in both
groups regardless of intervention. The significant de-
crease in narcotic consumption warrants a review of
clinical practice to incorporate cold therapy in the
standard postoperative order data set in this population.
Nurse attention and the continuance of regular turning
and positioning is also an important factor to continue,
as it may positively influence patient perceptions related
to pain. Independent clinical benefits associated with
turning and positioning bear further investigation.
table 2. change in nrs, pca use, anD perceiveD pain reDuction
Control Cold Therapy
Adjusted
Effect Size
n M ± SD n M ± SD
Difference in
means [95% CI] df
Chi-Square
Value
p
19. MPH; Michele Prigo, EdD; Bernard A. Rawlins, MD;
Andrew A. Sama, MD; and Kelsey Vukov, RN.
references
Abramson, D., Chu, L., & Tuck, S. (1966). Effect of tissue
temperatures and blood flow on motor nerve conduc-
tion velocity. JAMA: The Journal of the American
Medical Association, 198, 1082.
Adie, S., Kwan, A., Naylor, J., Harris, I., & Mittal, R. (2012).
Cryotherapy following total knee replacement.
Cochrane Database of Systematic Reviews, 9, 1–82.
Airaksinen, O. V., Kyrklund, N., Latvala, K., Kouri, J. P.,
Gronblad, M., & Kolari, P. (2003). Efficacy of cold gel
for soft tissue injuries: A prospective randomized dou-
ble-blinded trial. The American Journal of Sports
Medicine, 31(5), 680–684.
Amabile, C., & Bowman, B. (2006). Overview of oral modi-
fied-release opioid products for management of chronic
pain. The Annals of Pharmacotherapy, 40, 1327–1329.
Austin, P. C. (2009). Balance diagnostics for comparing the
distribution of baseline covariates between treatment
groups in propensity-score matched samples. Statistics
in Medicine, 28, 3083–3107.
Benyamin, R., Trescot, A., Datta, S., Buenaventura, R.,
Adlaka, R., Sehgal, N., … Vallejo, R. (2008). Opioid
complications and side effects. Pain Physician Journal:
Opioid Special Issue, 11, S105–S120.
Bleakley, C., McDonough, S., & MacAuley, D. (2004). The
use of ice in the treatment of acute soft-tissue injury: A
20. systematic review of randomized controlled trials. The
American Journal of Sports Medicine, 32(1), 251–261.
Block, J. (2010). Cold and compression in the management
of musculoskeletal injuries and orthopedic operative
procedures: A narrative review. The Journal of Sports
Medicine, 1, 105–113.
Brander, B., Munro, B., Bromely, L., & Hetreed, M. (1996).
Evaluation of the contribution to postoperative anal-
gesia by local cooling of the wound. Anaesthesia, 51,
1021–1025.
Fountas, K., Eftychia, K., Johnston, K., Smission, H.,
Vogel, R., & Robinson, J. (1999). Postoperative lumbar
micro discectomy pain. Spine, 24, 1958–1960.
Gordon, D. B., Stevenson, K. K., Griffie, J., Muchka, S.,
Rapp, C., & Ford-Roberts, K. (1999). Opioid equianal-
gesic calculations. Journal of Palliative Medincine, 2,
209–219.
Hjermstad, M. J., Fayers, P. M., Haugen, D. F., Caraceni, A.,
Hanks, G. W., & Loge, J. H. (2011). European Palliative
Care Research Collaborative (EPCRC). Studies com-
paring numerical rating scales, verbal rating scales,
and visual analogue scales for assessment of pain in-
tensity in adults: A systematic literature review.
Journal of Pain and Symptom Management, 41(6),
1073–1093. doi:10.1016/j.jpainsymman.2010.08.016
Konrath, G., Lock, T., & Goitz, H. (1996). The use of cold
therapy after anterior cruciate ligament reconstruc-
tion: A prospective randomized study and literature
review. American Journal of Sports Medicine, 24,
629–633.
21. Kullenberg, B., Ylipaa, S., Soderlund, K., & Resch, S.
(2006). Postoperative cryotherapy after total knee ar-
throplasty: A prospective study of 86 patients. The
Journal of Arthroplasty, 21(8), 1175–1179. doi:10.1016/j.
arth.2006.02.159
Lessard, L., Scudds, R., Amendola, A., & Vaz, M. (1997).
The efficacy of cryotherapy following arthroscopic
knee surgery. Journal of Orthopaedic & Sports Physical
Therapy, 26(1), 14–22.
Levy, A., & Marmar, E. (1993). The role of cold compres-
sion dressing in the postoperative treatment of total
knee arthroplasty. Clinical Orthopaedics, 297, 174–178.
Liu, S. S., Carpenter, R. L., Mulroy, M. F., Weissman, R. M.,
McGill, T. J., Rupp, S. M., & Allen, H. W. (1995).
Intravenous versus epidural administration of hydro-
morphone: Effects on analgesia and recovery after
radical retropubic prostatectomy. Anesthesiology,
82(3), 682–688.
Ma, Y., Mazumdar, M., & Memtsoudis, S. G. (2012). Beyond
repeated-measures analysis of variance: Advanced sta-
tistical methods for the analysis of longitudinal data in
anesthesia research. Regional Anesthesia and Pain
Medicine, 37, 99–105.
Murata, K., Yoshimoto, M., Takebayashi, T., Ida, K.,
Nakano, K., & Yamashita, T. (2014). Effect of cryother-
apy after spine surgery. Asian Spine Journal, 8(6), 753–
758. doi:10.4184/asj.2014.8.6.753
Schacht, A., Bogaerts, K., Bluhmki, E., & Lesaffre, E.
(2008). A new nonparametric approach for baseline
22. covariate adjustment for two-group comparative stud-
ies. Biometrics, 4, 1110–1116.
Stefee, A., Booher, J., & Biscup, R. (1996). Evaluation of
cold therapy in postoperative spine patients. Surgical
Technology, 5, 385–387.
Wahern, L., Torebjork, E., & Jorum, E. (1989). Central sup-
pression of cold-induced C-fiber pain by fiber myeli-
nated fiber input. Pain, 38, 313–319.
Wewers, M. E., & Lowe, N. K. (1990). A critical review of
visual analogue scales in the measurement of clinical
phenomena. Research in Nursing & Health, 13(4), 227–
236.
Wu, C. (2005). Acute postoperative pain. In R. D. Miller,
(Ed.): Miller’s anesthesia (6th ed., pp. 2745–2747).
Philadelphia, PA: Elsevier Churchill Livingstone.
Zeger, S., Liang, K., & Albert, P. (1988). Models for longitu-
dinal data: A generalized estimating equation ap-
proach. Biometrics, 44, 1049–1060.
** Adapted from: Rosswum: Image J Nurs Sch, Volume 31(4).
Fourth Quarter 1999.317-322
Kaiser Permanente Regional Nursing Research Committee;
modified June 2007
Topic: Journal
Author (Yr):
Title:
23. QUANTITATIVE REVIEW WORKSHEET
Purpose/Research
Questions/Hypotheses
Research
Variables Design Major Findings and Limitations
Purpose of Study: Independent: Quantitative Design: Findings:
(continue on back)
Research Questions /
Hypotheses: Dependent:
Theoretical Framework/
Conceptual Model:
Sample Setting Major Tools Limitations: (continue on back)
Number: Type: Name(s):
Type: #1
Age: #2
Gender: Location: #3 Levels of Evidence
Health Status: Urban or Rural Evidence Rating:
Statistics: Reliability:
Diagnosis: Descriptive: #1 Feasibility:
#2 Could this practice change be implemented easily
in
Other: #3 your organization and with minimal
resources?
24. Correlational: Yes No
Validity: Benefit/Risk:
#1 Would the benefits of the practice change outweigh
Inferential: #2 the risks to patients? Yes No
#3
Comments:
Statistics:Benefit/Risk:
PrintButton1: TextField1: DropDownList1: Select
One:DropDownList2: Evidence Level: Select Evidence
Rating:DropDownList3: Select Method:CheckBox1:
0CheckBox2: 0CheckBox3: 0CheckBox4: 0CheckBox5:
0CheckBox6: 0TextField2: TextField3:
NUR 440 Critique Guidelines and Rubric
Overview: When caring for patients it is essential that as a
nurse you are using evidence-based practice. In order to identify
what is best practice, you must be
able to read research critically. Terminology used in research
can be difficult to interpret and understand; therefore securing a
solid foundation is essential to the
success of identifying and implementing current best practice.
What is a critique? It is a professional analysis of the
weaknesses and strengths of a particular
piece of research. A critique may be done for a variety of
purposes: acting as an expert reviewer to assess whether this
research paper should be published;
providing helpful comments on a work before it is submitted for
25. publication; or, as in the case here, as a learning experience for
emerging scholars to practice
their developing research skills.
Prompt: Choose one of the two provided articles located in the
module Reading and Resources folder. Start by filling out the
provided worksheet. Then, using the
worksheet as your guide, write a critique to dig deeper into each
section and identify the specific examples of each element (e.g.,
what is the research question?
Does the author justify the importance of the research? In the
case of a literature review, has the author examined the relevant
literature?). Elaborate on each
section and evaluate it for its strengths and limitations. Be sure
to identify your chosen article and address the following critical
elements:
x Critique
o Purpose and Research Question: What is the research
question? Does the author justify the importance of the
research?
o Design and Methods: What design and methods were used?
Are they rigorous and systematic?
o Validity and Reliability: Is the study valid and reliable? (For
qualitative research, this section of your critique should
consider the study’s
trustworthiness and rigor.)
o Findings and Conclusions: Are the conclusions reasonable
given the findings?
x Evaluation: What are the strengths and weaknesses of the
research article? Do you agree with the author’s conclusions?
Why or why not? Did the author
succeed or fail in the purpose of the study? Recommend areas
26. for improvement or suggest direction for future research.
Guidelines for Submission: Your paper must be submitted as a
1–2 page Microsoft Word document with double spacing, 12-
point Times New Roman font, one-
inch margins, and in APA format.
Critical Elements Exemplary (100%) Proficient (85%) Needs
Improvement (55%) Not Evident (0%) Value
Critique Meets “Proficient” criteria and
includes examples from the
article and an insightful
discussion of validity and
reliability or trustworthiness
and rigor where applicable
Critiques each section identified
above and elaborates by using
content from the course;
includes a discussion of validity
and reliability or
trustworthiness and rigor
where applicable
Briefly critiques most of the
sections identified above but
does not discuss validity and
reliability or trustworthiness
and rigor where applicable
Does not critique any of the
sections
27. 45
Evaluation Meets “Proficient” criteria and
offers insightful suggestions for
improvement or direction of
future research
Evaluates the research article
for its overall strengths and
weaknesses and offers
suggestions for improvement or
direction for future research
Briefly evaluates the research
article for its overall strengths
and weaknesses and does not
offer suggestions for
improvement or direction for
future research
Does not evaluate the research
article
45
Articulation of
Response
(APA/Mechanics)
Submission is free of errors
related to citations, grammar,
28. spelling, syntax, and
organization and is presented in
a professional and easy-to-read
format
Submission has no major errors
related to citations, grammar,
spelling, syntax, or organization
Submission has major errors
related to citations, grammar,
spelling, syntax, or organization
that negatively impact
readability and articulation of
main ideas
Submission has critical errors
related to citations, grammar,
spelling, syntax, or organization
that obstruct understanding
10
Earned Total 100%