This document discusses several common pediatric respiratory problems. It begins by outlining signs of respiratory distress and failure in children, including increased respiratory rate and heart rate, nasal flaring, recession of the chest wall, and decreased oxygen saturation despite supplemental oxygen. Specific conditions are then discussed such as croup, epiglottitis, bronchiolitis, pneumonia, whooping cough, inhaled foreign bodies, cystic fibrosis, and heart failure. For each condition, the causes, signs and symptoms, investigations, and management are summarized. The document provides an overview of approaches to evaluating and treating major respiratory issues seen in pediatric patients.
3. Respiratory distress:
↑RR and ↑HR.
Nasal flaring.
Agitation
Recession/retraction: subcostal (milder), intercostal
(moderate), sternal (severe).
Accessory muscle use (scalene, SCM) and head bobbing
(severe).
Grunting: expiratory noise due to an attempt to maintain
PEEP (severe).
5. DDx: Cough in children
Infection
Asthma, allergic rhinitis.
2nd hand smoke.
Inhaled foreign body, aspiration.
CF
Habit cough.
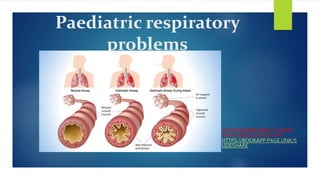
6. DDx: Wheeze in children
Wheeze – a coarse, expiratory whistling sound –
suggests lower respiratory tract problems:
Infection: bronchiolitis, pneumonia.
Allergic: asthma, milk allergy.
Transient early wheeze, viral wheeze.
Severe disease: heart failure, CF.
Inhaled foreign body and/or aspiration pneumonia.
Tracheomalacia (and/or stridor).
7. DDx: Stridor in children
Stridor – a harsh, high pitched sound which is usually
inspiratory – suggests upper respiratory tract problems:
Infection: croup, bacterial tracheitis, epiglottitis.
Anaphylaxis
Inhaled foreign body.
Laryngomalacia
Tracheomalacia
8. DDx: Respiratory crackles in
children
Fine crackles point to inflammation in the smaller airways –
bronchioles – while coarse crackles point to bronchial
involvement.
Usually inspiratory, but they can be expiratory too if there
are voluminous secretions.
Bronchiolitis causes bilateral, fine end inspiratory crackles.
Pneumonia causes uni- or bilateral coarse crackles.
9. Investigations
Chest X-ray
Procedure and indications
Often supine AP
, as it may be difficult to get an erect PA.
If clinical diagnosis is clear, there is often no need for CXR
in children. More likely to be useful when there is
uncertainty e.g. younger kids with vague symptoms.
10. Findings
Pneumonia:
Consolidation: lobar if Strep. pneumo.
Cavitation if Staph. aureus or TB.
Pleural effusion/empyema.
Severe bronchiolitis → hyperinflation:
>6 anterior ribs.
Flat diaphragm.
11. Others:
Inhaled foreign body: requires inspiratory and
expiratory film. Hyperlucent object and collapse
distal to it.
CF: bronchiectasis shadowing.
HF: hyperinflation, cardiomegaly.
12. Other investigations
Detecting pathogens:
Nasal swabs can pick up respiratory viruses e.g. RSV.
Nasopharyngeal aspirate is more accurate but more
invasive.
Blood gas:
In neonates and infants capillary blood can be used,
though the O2 readings are not very useful.
14. Croup
Acute laryngotracheobronchitis with subglottic
inflammation and oedema.
Epidemiology and causes
Viral URTI due to parainfluenza 1-4 (80%), RSV, and
various rare causes.
6 months to 6 years of age, commonest age 1-2.
Highest prevalence in autumn.
17. Bacterial tracheitis
Bacterial infection of trachea. Increased risk following viral
URTI due to mucosal damage and local immune changes.
Pathogens
Staph. aureus.
Haemophilus influenzae type b (Hib).
Strep. pneumo.
18. Signs and symptoms
Stridor
Purulent secretions.
Mucosal necrosis and sloughing.
High fever.
Management
IV antibiotics.st
Epiglottitis
19. Epidemiology and causes
Haemophilus influenzae type b (Hib) is traditionally the
commonest cause, but becoming less so due to the Hib
vaccine. Other causes include the usual respiratory
pathogens such as Strep. pneumo.
Commonest in kids age 1-6 years, especially 2-3 years.
Incidence is falling in kids, due to Hib vaccine, but rising in
adults.
20. Signs and symptoms
Acute onset of high fever, sore throat, and drooling (can't
swallow secretions).
Stridor: soft and continuous. A late sign suggesting airway
obstruction.
Whispering
Tripoding: sitting up and leaning forward on outstretched
arms to ease upper airway obstruction.
In adults, onset is more gradual.
21. Management
Get senior help from anaesthetics, paediatrics, and/or ENT.
Oxygen or heliox can be given in the meantime, but do
not disturb child with oral examination or trying to gain IV
access, as it may precipitate respiratory distress. If there is
airway compromise, nebulised adrenaline can buy a small
amount of time before the airway is secured.
22. Management
Definitive treatment requires intubation and IV antibiotics.
Intubation is often not needed in adults.
Diagnosis is usually made by laryngoscopy during
intubation. In patients who are not intubated, a lateral
neck XR showing the thumb print sign can aid diagnosis.
Investigations like blood culture and neck swabs can be
safely done once airway is secure.
23. Bronchiolitis
Infection of the bronchioles, usually viral.
Epidemiology and causes
Pathogens: RSV (75%), parainfluenza, human
metapneumovirus, adenovirus (often severe).
Commonest in kids
25. Signs and symptoms
1-3 days coryzal prodrome with clear secretions.
Wet or dry cough.
Respiratory distress. Apnoea may occur if
Fever, though usually <39°C.
Poor feeding and dehydration.
On auscultation: wheeze, bilateral fine end-
inspiratory crackles.
26. Investigations
Diagnosis usually clinical.
O2 sats to assess severity.
PCR of nasopharyngeal aspirate can confirm
pathogen but not routinely indicated.
Bloods, blood gas, and CXR not routinely
recommended, unless severe disease and/or
other etiology (e.g. pneumonia) suspected.
27. Management
Management is usually conservative.
Suction secretions if causing respiratory distress or feeding
difficulties, or if there is apnoea.
If O2 sats are low, give humidified O2 through nasal
cannula or headbox.
If respiratory failure impending, consider CPAP or
mechanical ventilation.
Evidence is ambiguous on benefits of nebulized
hypertonic saline. No evidence to support use of
bronchodilators, steroids, or antibiotics.
28. Viral-induced wheeze
Wheeze following a viral infection such as
bronchiolitis.
Often responds to bronchodilators.
If it persists beyond a few weeks, child may be
more likely to go on to get an asthma diagnosis
when over 2 years old.
32. Signs and symptoms
General URTI signs 1st.
High fever.
Respiratory distress.
Malaise and poor feeding.
Auscultation: bronchial breathing and unilateral
coarse end-inspiratory crackles.
Pathogen-specific signs: wheeze if viral or
mycoplasma, abdo or neck pain if bacterial.
33. Management
Amoxicillin PO 7 days.
IV if very young or very ill.
Whooping cough
Pathogen and epidemiology
Bordetella pertussis, a gram-negative coccobacillus.
Accounts for 20% of persistent coughs (>2 weeks) in
school-age kids, even if vaccinated.
34. Clinical features
Typical URTI 1st.
Followed by a paroxysmal stage: episodes of
prolonged hacking cough then inspiratory
whoop, possibly accompanied by red face,
bulging eyes, vomiting, or syncope. May be
triggered by a startle, and often worse at night.
Can last up to 3 months.
35. Management
Macrolide PO if
Prophylactic macrolide to all household
contacts if any one of them is high risk:
infants with 32 weeks, work with infants or
pregnant women.
Can return to school 5 days after starting
antibiotics.
36. Inhaled foreign body
Signs and symptoms
Classic triad:
Persistent cough following choking episode.
However, initial choking is missed in 20%, so
symptoms can last for weeks before diagnosis.
Wheeze
↓Lung sounds.
37. Investigations and management
CXR, though only 25% of inhaled items are
radiopaque.
If location known, rigid bronchoscopy under general
anaesthetic (GA) to remove it.
If location unknown, flexible bronchoscopy under
sedation to find it, then rigid bronchoscopy under
GA to remove it.
38. Complications
Complete airway obstruction.
Pneumonia. Can be recurrent and lead to
abscesses and bronchiectasis.
Pneumothorax
Lobar collapse.
40. Genetics and pathophysiology
Autosomal recessive mutation in CFTR gene on
chromosome 7, most commonly (70%) ΔF508. 1/25 of UK
population are carriers.
CFTR is an apical chloride channel. Chloride movement
across cell membranes is often followed by Na+ and H2O.
Pancreatic interlobular ducts also become clogged with
mucus, leading to impaired secretion of digestive enzymes
and eventually pancreatic destruction.
41. Genetics and pathophysiology
In upper airways, CFTR dysfunction leads to
reduced fluid flow into airways and hence failure
of mucus to be cleared. This leads to recurrent
pneumonia from Staph. aureus, H.
influenzae, Strep. pneumo, and eventually
chronic Pseudomonas aeruginosa, as well as
bronchiectasis.
In sweat glands, impaired chloride removal from
the duct (and hence Na+) leads to salty sweat.
42. Presentation
Recurrent pneumonia is the commonest
presentation. Staph. aureus is the most
common dangerous pathogen in kids,
and Pseudomonas aeruginosa later.
Neonatal meconium ileus: failure to pass the
tar-like first stools of neonates. The presenting
complaint in 10%.
Other GI: steatorrhea, rectal prolapse, small
bowel obstruction, GORD, PUD.
43. Presentation
Slow growth.
Clubbing
Nasal polyps, sinusitis.
Later, male infertility due to congenital bilateral
absence of the vas deferens (CBAVD), leading to
obstructive azoospermia.
10% diagnosed age ≥16, typically presenting with
pulmonary, sinus, or fertility issues.
44. Differential diagnosis
A chronic wet cough or recurrent/prolonged
pneumonias may also be caused by:
Immunodeficiency: congenital, HIV.
TB
Other causes of bronchiectasis e.g. primary ciliary dyskinesia.
45. Investigations
Newborn screening picks up most cases. Diagnosis is
then confirmed by combination of 2 tests:
Sweat test showing ≥60 mmol/L chloride. Consider further
investigations if 40-59 mmol/L.
Genetic testing showing 2 disease-causing mutations (i.e. both
alleles). Initially checks for common mutations, with option of
further sequencing if necessary.
46. Other tests:
CXR
PFT: FEV1 is a key prognostic factor.
Sputum culture.
Management
MDT:
Specialist consultants, nurses, physiotherapists,
dieticians, social workers, and psychologists.
47. Respiratory:
Mucus clearance: chest physio (postural drainage,
percussion and vibration, forced expiration) and nebulized
mucolytics (dornase alfa [a DNAse], hypertonic saline,
mannitol).
Anti-microbials: prophylactic inhaled tobramycin (if age ≥6
with chronic P
. aeruginosa), and high-dose long-course
antibiotics when treating infections.
Anti-inflammatories (if age ≥6): long-term azithromycin or
ibuprofen.
Bilateral lung transplant if medical therapy fails.
48. Non-respiratory:
If there is pancreatic insufficiency (>80%), give
enteric-coated pancreatic enzymes before each
meal.
Nasal polyps may require steroids or surgery.
Targeted therapy:
Ivacaftor and lumacaftor are novel CFTR modulators with
modest effects on lung function and exacerbation
frequency. Availability currently limited by price.
49. Complications
Respiratory failure, pulmonary HTN, and cor pulmonale.
Diabetes
Osteoporosis
Cirrhosis
Prognosis
Predicted median survival 40-50 years if
born today.st
51. Causes and epidemiology
A number of structural heart defects can lead to
heart failure, including VSD, PDA, coarctation of
the aorta, and valve disease. See congenital heart
disease.
Arrhythmias and myocardial disease can also be a
cause.
Most commonly presents in the first 3 months.
53. THANK YOU
Thank you for visiting this slide. Keep
supporting Medicos PDF. Medical student can
download any books from Medicos PDF app
as well as we can upload our own slides for
free. Visit app from
https://bookapp.page.link/slideshare