
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Myeloma & spep interpretation Marwa Khalifa
Similar to Myeloma & spep interpretation Marwa Khalifa (20)
More from Marwa Khalifa
More from Marwa Khalifa (20)
Recently uploaded
Recently uploaded (20)
Myeloma & spep interpretation Marwa Khalifa
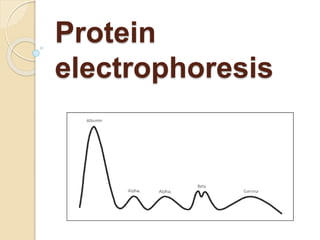
- 2. Serum is placed on a specific medium, and a charge is applied. Differentiation :net charge (positive or negative) and the size and shape of the protein Total protein - 6.4-8.3 g/dL Albumin - 3.5-5 g/dL Globulin - 2.3-3.4 g/dL Alpha-1 globulin - 0.1-0.3 g/dL Alpha-2 globulin - 0.6-1 g/dL Beta globulin - 0.7-1.1 g/dL
- 3. Components ALBUMIN ALPHA FRACTION: alpha1-protein fraction is comprised of alpha1-antitrypsin, thyroid-binding globulin, and transcortin. Ceruloplasmin, alpha2-macroglobulin, and haptoglobin contribute to the alpha2-protein Liver disease Acute inflammation, malignancy
- 4. BETA FRACTION: two peaks labeled beta1 (transferrin) and beta2 (beta- lipoprotein) +/- IgA, IgM, and sometimes IgG, complement Cirrhosis /Carcinoma/Cushing’s Diabetes mellitus /Hypothyroidism IDA/ Malignant hypertension Nephrosis /Polyarteritis nodosa /Obstructive jaundice /3rd tri pregnancy
- 5. GAMMA FRACTION: immunoglobulins IgG type. The gamma-globulin zone is decreased in hypogammaglobulinemia and agammaglobulinemia. monoclonal gammopathy : Myeloma Waldenström’s macroglobulinemia, solitary plasmacytoma, smoldering multiple myeloma, MGUS, plasma cell leukemia, heavy chain disease, and amyloidosis
- 6. Polyclonal Gammopathy 1. Viral hepatitis, HIV, mononucleosis, and varicella 2. bacterial infections: endocarditis, osteomyelitis, and bacteremia Tuberculosis 3. Connective tissue diseases SLE Mixed connective tissue Temporal arteritis RA Sarcoid 4. Liver diseases: alcohol Cirrhosis hepatitis biliary cirrhosis Primary sclerosing cholangitis
- 10. Indications Suspected multiple myeloma, Waldenström’s macroglobulinemia, primary amyloidosis, or related disorder Unexplained peripheral neuropathy (not attributed to longstanding diabetes mellitus, toxin exposure, chemotherapy, etc.) New-onset anemia associated with renal failure or insufficiency and bone pain Back pain in which multiple myeloma is suspected Hypercalcemia attributed to possible malignancy (e.g., associated weight loss, fatigue, bone pain, abnormal bleeding) Rouleaux formations noted on peripheral blood smear Renal insufficiency with associated serum protein elevation Unexplained pathologic fracture or lytic lesion identified on radiograph Bence Jones proteinuria
- 13. 1.8% of all cancers 17% of all haematological malignancies median age at diagnosis of 69 years Diagnosed among people 65-74y
- 14. Diagnostic Criteria 2014 IMWG criteria Clonal bone marrow plasma cells ≥ 10% or biopsy-proven bone or extramedullary plasmacytoma Any one or more of the following myeloma-defining events Hypercalcemia (greater than upper limit of normal) Renal insufficiency: serum creatinine >2 g/dL or creatinine clearance <40 mL/min Anemia: hemoglobin <10 g/dL or 2 g/dL below lower limit of normal Bone lesions: one or more osteolytic lesions (as demonstrated on imaging studies) New criteria Involved/uninvolved serum free light chains ratio ≥ 100, and the involved serum free light chain level ≥ 100 mg/dL Clonal bone marrow plasma cells ≥ 60% ≥ 2 focal lesions based on MRI studies of the skeleton
- 15. Work up Serum and/or urine protein electrophoresis (24h urine collection) : M band Quantification of IgG, IgA, IgM immunoglobulins; Immunofixation; and serum-free light chain (FLC) measurement. Bone marrow :plasma cell infiltration , cytogenetics, flowcytometry CBC: rouleaux formation serum creatinine, creatinine clearance and calcium LDH , B2M, albumin
- 16. Lytic bone lesions: whole-body low- dose computed tomography (WBLD- CT). Conventional radiography if WBLD-CT is not available MRI used in selected situations (eg, risk stratifying smoldering myeloma, for monitoring response of nonsecretory and oligosecretory myeloma, and if CT or skeletal survey is inconclusive)
- 17. Cytogenetics 17p del T(4,14), t(14,16), t(14,20) 13q del 1p del, 1q amplification
- 18. Staging
- 19. Treatment Transplant eligible or not ?? eligibility criteria for ASCT? Chronologic age and renal function should not be the sole criteria used to determine eligibility for SCT
- 20. What are the options for initial therapy before transplant? at least three to four cycles of induction therapy including an immunomodulatory drug, proteasome inhibitor (PI), and steroids achieving at least very good partial response (VGPR) Up-front transplant should be offered to all transplant-eligible patients. improved PFS
- 21. TRANSPLANT-INELIGIBLE POPULATION Multiple factors should be considered; disease-specific factors such as stage and cytogenetic abnormalities, and patient- specific factors including age, comorbidities, functional status, frailty status, and patient preferences should include at minimum a novel agent (immunomodulatory drugs or PI) and a steroid if possible The combination of thalidomide, melphalan, and prednisone, combination of bortezomib, melphalan, and prednisone Daratumumab plus bortezomib plus melphalan plus prednisone may also be
- 22. Drugs Used in the Treatment of Patients With Multiple Myeloma
- 26. Mechanism of PI PIs suppress the production of cytokines (IL-6), (IGF-1), (TNFα), which can affect MSC and myeloma cell interactions. PIs suppress angiogenesis by decreasing VEGF secretion. PIs allow for the accumulation of misfolded and unfolded proteins, resulting in endoplasmic reticulum (ER) stress, reactive oxygen species (ROS)- induced oxidative stress, and the
- 27. PIs inhibit NF-κB signaling, a major growth and survival signaling pathway in MM PIs upregulate p53, a tumor suppressor to induce cell cycle arrest. PIs can induce apoptosis through extrinsic caspase-8 cascade , and via caspase-9 cleavage. PIs suppress adhesion molecule and growth factor receptor expression (e.g., IL-6R) and inhibit cellular mechanisms for repairing double-strand DNA breaks
- 30. increasing use of immunomodulatory drugs, lenalidomide in particular, (beyond four to six cycles) may also compromise stem-cell yield.
- 31. Tandem or not tandem ? A single ASCT is considered the standard of care based upon the randomized BMT Clinical Trial Tandem ASCT should not be routinely recommended High-dose melphalan is the recommended conditioning regimen for ASCT
- 32. Role of Allo not routinely recommended but may be considered in select high-risk patients or in the context of a clinical trial
- 33. Consolidation and Maintaince Consolidation therapy is not routinely recommended For patients ineligible or unwilling to consider maintenance therapy, consolidation therapy for at least two cycles may be considered. Lenalidomide maintenance therapy should be routinely offered to standard-risk patients starting at approximately day 90 to 110 at 10 to 15 mg daily until progression. A minimum of 2 years of maintenance therapy is associated with improved survival
- 34. For patients intolerant of or unable to receive lenalidomide, bortezomib maintenance every 2 weeks may be considered For high-risk patients, maintenance therapy with a PI with or without lenalidomide may be considered
- 36. RELAPSED DISEASE should be treated immediately A triplet regimen with two novel agents (PI, immunomodulatory drug, or monoclonal antibody) in combination with a steroid A monoclonal antibody–based regimen in combination with an immunomodulatory drug and/or PI should be considered. Treatment of relapsed multiple myeloma may be continued until disease
- 39. Transplant post relapse ASCT, if not received after primary induction therapy, should be offered to transplant eligible Repeat SCT may be considered in relapsed multiple myeloma if PFS after first transplant is ≥ 18 months Allogeneic hematopoietic cell transplantation has the potential of producing cure (TRM, GVHD)
- 41. Bone disease 80% Pamidronate is administered at a monthly dose of 90mg via a 2 h i.v. infusion. Zoledronic acid at a monthly dose of 4mg administered via a 15 min infusion. In patients with creatinine clearance 30– 60 mL/min, the dose of zoledronic acid must be reduced to a maximum of 3mg Patients with hypercalcaemia should also receive zoledronic acid osteonecrosis of the jaw.
- 42. IMWG and the ASCO do not recommend the initial use of bisphosphonates for more than 2 years. In relapsed patients, treatment with bisphosphonates can be restarted and administered concomitantly with active therapy.
- 43. spinal cord compression emergency that requires treatment with high-dose dexamethasone and simultaneous local radiotherapy should be started as soon as possible;
- 44. Anaemia, BM failure and infections Recombinant human erythropoietin and darbepoetin alfa can be used for the treatment of myeloma-associated anaemia (haemoglobin level < 10 g/dL), once other causes of anaemia have been excluded . The target is to maintain haemoglobin around12 g/dL (below 14 g/dL to avoid thromboembolic complications and hypertension)
- 45. G-CSF may be required to treat chemotherapy-induced severe granulocytopaenia. Infectious episodes require immediate therapy with broad spectrum antibiotics. Prophylaxis of infection controversial ,first 2–3 months of initiation of lenalidomide or pomalidomide, or in patients at high risk of infection
- 46. IVIG for recurrent life threatening infection Influenza and pneumococcal vaccinations are recommended Acyclovir or valacyclovir for herpes- zoster virus prophylaxis is recommended for patients receiving proteasome inhibitor-based therapies
- 47. Renal impairment 33% Bortezomib-based therapies (in combination with dexamethasone thalidomide or doxorubicin or cyclophosphamide is the treatment of choice in patients with renal failure
- 48. Venous thromboembolism. Increased risk of thrombosis 3%–4% High-dose dexamethasone, cytotoxic chemotherapy such as doxorubicin and IMiDs (thalidomide and lenalidomide) increase this risk The current recommendations for patients with MM who are due to start IMiD therapy are to use aspirin (81-325 mg) in the absence of risk factors for thrombosis and to use full dose anticoagulants for those at higher risk
- 49. Hypercalcemia Hydration Bisphosphonate Denosumab Steroids
- 50. Non-Secretory Myeloma: Ready for a new Definition? monoclonal plasma cells ≥10% in the bone marrow and by negative results on serum and urine electrophoresis and immunofixation studies. evidence of end-organ damage Either non producer or non secretors
- 51. Oligo-secretory “free light only” myeloma light chain myeloma serum protein of < 1.0 g/dL, urine protein of < 200 mg/24 hrs, and free light chain values of < 100 mg/L
- 52. Solitary Plasmacytoma existence of a histologically confirmed solitary plasma cell tumour either osseous or extraosseous in the absence of BM infiltration and CRAB symptoms Local radiotherapy is the preferred treatment of choice 30-60 Gy, but about two-thirds of patients develop MM at 10 years’ follow-up Follow up 3-6 m
- 53. Plasma cell leukaemia Poor outcomes OS≈ 1y >20% clonal plasma cells in peripheral blood or >2 × 109 /l no specific treatment approaches for PCL. The use of multidrug combinations (including both a proteasome inhibitor and an IMiD) followed by HDT in eligible patients, followed by prolonged maintenance until progression
- 54. POEMS syndrome