Nursing Management of patient undergoing renal transplantation.pdf
•
0 likes•1,171 views

renal transplantation

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Nursing Management of patient undergoing renal transplantation.pdf
Similar to Nursing Management of patient undergoing renal transplantation.pdf (20)
More from karna ram choudhary
Recently uploaded
Recently uploaded (20)
Nursing Management of patient undergoing renal transplantation.pdf
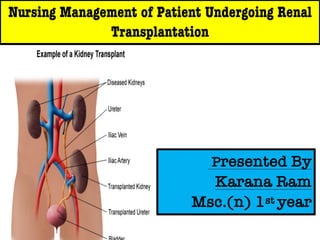
- 1. Nursing Management of Patient Undergoing Renal Transplantation Presented By Karana Ram Msc.(n) 1st year
- 3. INTRODUCTION ➢Renal transplantation is the treatment of choice for chronic irreversible renal failure. ➢The current donation rate is much higher in the four states of Tamil Nadu, Andhra Pradesh, Gujarat and Maharashtra with it being 0.3 per million population
- 4. ➢Definition ➢ Renal transplantation is the surgical implantation of a Human kidney from a compatible donor in a recipient”. OR ➢A kidney transplant is a surgery to place a healthy Kidney from a living or deceased donor into a person Whose kidneys no longer function properly.
- 5. History ➢1902- The first successful experimental kidney transplants were performed at the Vienna Medical School in Austria with animals. ➢1909 - The first kidney transplant experiments were performed humans in France using animal kidneys. ➢1933 - The first human-to-human kidney transplant was performed. ➢1950 - Cortisone-like medications were used to suppress the human body immune system resulting kidney transplant success.
- 6. INDICATION ➢ ESRD ➢Chronic glomerulonephritis ➢Chronic pyelonephritis ➢Solitary functioning kidney as a result of trauma ➢Renal cancer ➢Genetics disease- polycystic kidney diseases. ➢Chronic renal failure (CRF).
- 7. DONOR Selection of donor - ➢Age : 2 -70 years ➢Free from diseases. ➢Kidneys should be capable of good function
- 8. TYPES OF DONOR ➢Living donor ➢Cadaver donar ➢Non-heart-beating donors
- 9. Preoperative Diagnosis Basic Investigation are- CBC, KFT, SGPT, S.ALBUMIN, CALCIUM/PO4, LDH, BLOOD SUGAR ,HbA1c,TSH, PT/ APTT ,HbS Ag, Anti HCV, LIPID PROFILE, URINE MICROSCOPY, URINE CULTURE, 24 hour urine Protein, ECG,, USG whole Abdomen, Chest X-Ray, Blood Grouping, GFR. • DTPA Scan OF RECIPIENT ASAP (date with in 2 weeks) • Rh incompatibility • Abo incompatibility • Platelet different study • HLA testing.
- 10. PRE-OPERATIVE/CHECKLIST- 1. VBG- Post Haemodialysis after admission 2. CBC, KFT, PT /APTT,. 3. Blood Grouping and cross matching. 4. ECG. S. Nil orally. 6. Part preparation . 7. P.C. enema 8. Betadine paint 10. Written Consent ,11. Injection Emeset 12. Injection Augmentin- Dose: 600 mg IV BD 13. Injection Magnex forte 1.5 gm IV 14.Cap. Tacrolimus 16. Tab. Mofetyl S 720 mg 17. Tab. Ativan- 1mg 18. Injection rabbit ATG 75 MG 19. Injection Augmentin, Injection Magnex forte to be sent with patient in OT. 20. Recipient's arterial line, central line ON LEFT IJV
- 11. CONTRAINDICATION Active malignancy Active infection Peripheral vascular disease Severe cardiac or pulmonary disease Active IV drug abuse
- 12. MEMBER OF RENAL TRANSPLANT TEAM Transplant Surgeons. Transplant Nephrologists. Transplant Coordinators. Transplant Fellows and Residents Transplant nursing officer Other supportive staff.
- 14. DONOR Client placed in lateral decubitus position Incision made at level of 11th rib. The left kidney mostly preferred for laparoscopic removal.
- 15. HTK- Custodial Solution HTK (Histidine- Tryptophan-Ketoglutarate) Solution. HTK is perfused as a cold solution, so that its hypothermic effect contributes to a decreased metabolic rate.
- 16. RECIPIENT Incision made between iliac crest and pubis. Transplanted kidney placed in iliac fossa.
- 17. Contd,, Renal artery anastomosed with external iliac artery and renal vein with external iliac vein. Donor ureter anastomosed with bladder mucosa
- 19. Preoperative Management •A complete physical examination is performed to detect and treat any conditions that could cause complications after transplantation. •The patient must be free of infection at the time of renal transplantation because after surgery the patient will receive medications to prevent transplant rejection. •Hemodialysis is often performed the day before the scheduled transplantation •Provide psychological support to the patient.
- 20. Contd,, • Patient should be NPO for 6 hours before surgery. • Informed consent should be taken from patient as well as relatives also. • Antibiotic should be given before surgery as prescribed by surgeon. • Skin preparation of operating site should be done.
- 21. POST OPERATIVE MANAGEMENT ❑ Immunosuppressive therapy- glucocorticoid calcineurine inhibitor purine antagonist
- 22. GLUCOCORTICOID Eg: prednisolone Maintenance dose: 10 to 15 mg per day SIDE EFFECTS : Impaired wound healing Infection
- 23. CALCINEURIN INHIBITORS Eg: cyclosporine , tacrolimus Dose : 6-8 mg/ kg per day SIDE EFFECTS :. Nephrotoxicity Glucose intolerance Hypertention Gingival hyperplasia
- 24. PURINE ANTAGONIST Azathioprine (Azoran) DOSE: 1.5 to 2 mg/kg per day ACTION: Inhibits both DNA & RNA synthesis and prevents growth of lymphocytes Side effects ●Neutropenia (main) ●Alopecia ●Muscular pains ●Malignancy ●Altered liver function
- 25. POSTOPERATIVE NURSING MANAGEMENT Maintaining the normal blood pressure. Assessing the surgical site. Blood sugar monitoring 4 hourly. Maintain strict aseptic precautions and Preventing from infection Monitoring and managing potential complication. Strictly monitor urine output hourly. Assessing the patient from transplant rejection. Replace the urine output with IV fluid. Vaccinated the patient.
- 26. POST OPERATIVE NURSING DIAGNOSIS INEFFECTIVE AIRWAY CLEARANCE RELATED TO DEPRESSED RESPIRATORY FUNCTION, PAIN, AND BED REST ➢Close monitoring of respiratory status. ➢Assess respiratory pattern, auscultate for any crackles or abnormal respiratory sounds ➢Early chest physiotherapy ➢Encourage to do deep breathing exercises
- 27. RISK FOR FLUID AND ELECTROLYTE IMBALANCE RELATED TO POTENTIAL GRAFT DYSFUNCTION ➢Assess CVP and urine output hourly. ➢Fluids given are 5% dextrose, RL, NS. administered through central venous line. ➢Oral fluids are given once the patient tolerates. ➢ Amount of fluid to be given ➢Output less than 50ml/hr : inform ➢Output 50- 200ml/hr: output+150ml ➢Output 200-400ml/hr: output amount ➢Output 400-500ml/hr:400ml of fluid
- 28. ACUTE PAIN RELATED TO SURGICAL SITE INCISION Assess pain : patterns, any radiating pain. Administer analgesics as prescribed ●Epidural analgesia or PCA Opiate derivative- morphine is commonly used ●Non pharmacological measures like distraction, imagery, relaxation etc can be used.
- 29. RISK FOR TRANSPLANT REJECTION IN THE RECIPIENT RELATED TO NON HISTOCOMPATIBILITY Assess for oliguria, edema , fever, increase BP, weight gain, and swelling or tenderness over graft.
- 30. POTENTIAL FOR DEVELOPING INFECTION RELATED TO THE IMMUNO SUPPRESSED STATE ➢Assess for infection: chills and fever, tachycardia, tachypnea & decrease or increase in WBC count ➢Strict hand hygiene & use of barrier nursing ➢Meticulous care of urinary catheter, wound, peritoneal catheter site & CVP line using aseptic technique. ➢Visitors are minimized and monitored for infections ➢Maintain patient’s personal & oral hygiene
- 31. DISCHARGE TEACHING ▪ Educate them about the need for continuing immunosuppressive therapy. ▪ Instruct family members to assess for signs and symptoms of transplant rejection, infection, & potential adverse effect of immunosuppressant medication. ▪ Explain the patient need for life long follow up care. ▪ Avoid long time sitting, ▪ Watch for malignancy as the patient is receiving long term immunosuppressive therapy.
- 32. DIETARY MODIFICATIONS ➢ Limit sodium, saturated fat and cholesterol intake. ➢ Monitor weight on a daily basis. ➢ Avoid sugary snacks between meals ➢ Eat 1000- 1500mg calcium daily ➢ Regular exercise 30 mins at least 3 times a week ➢ Drink plenty of fluids 3 to 4 litres per day
- 33. Clinic visits ➢ Upto 2 months : twice a week ➢ 3 to 6 month : once a week ➢ 6 to 1 yr : once a month ➢ More than 1 yr : Atleast once in 3 months Lab tests ➢ Test for kidney function ➢ Test for blood count ➢ Test for liver function ➢ Blood glucose
- 34. PROGNOSIS ▪ 1 year graft survival rates are 85% to 90% with transplants from living donors and 75% to 80% with cadaver kidneys ▪ The overall mortality rate 2 year after transplantation is about 10%
- 35. COMPLICATION ❑ Infection ❑ Rejection ❑ Cardiovascular disease ❑ Renal artery stenosis ❑ Blood clots and bleeding ❑ Corticosteroid related complications
- 36. GRAFT REJECTION Sign and symptoms- •Temperature higher than 100 °F (37.8 °C) •Pain or tenderness over the grafted kidney • 2- to 3-lb weight gain in 24 hours •Edema •Hypertension •Elevated blood urea nitrogen and serum creatinine levels Decreased creatinine clearance Elevated white blood cell count
- 37. TYPES Hyperacute rejection- Hyperacute rejection occurs immediately in the operating room or within 48 hours after the transplant. Intervention:- Removal of rejected kidney
- 38. ACUTE REJECTION Occurs within 1 week postoperatively, but can occur any time post transplantation. Intervention: Potentially reversible with increased immunosuppressive therapy and corticosteroids.
- 39. CHRONIC REJECTION Occurs slowly months to years after transplant(Gradual decline in renal function.) Associated with renal ischemia, hypertention, tubular atrophy, interstitial fibrosis. Can be due to HLA incompatibility, age, and ischemic history of a donor kidney. Interventions: Immunosuppressive medications and dialysis if necessary.
- 40. RESEARCH ARTICLE A Study on the Correlations of Anxiety and Depression With Self-Management Ability and Endogenous Creatinine Clearance Rate in Renal Transplant Recipients
- 41. ABSTRACT Objective: To explore the e ff ects of anxiety and depression on the self-management ability and endogenous creatinine clearance rate of renal transplant patients. Method: Eighty-eight renal transplant recipients who were followed up in the outpatient clinic of the A ffi liated Hospital of Zunyi Medical University were selected using convenient sampling. The self-made general data sheet, Self-Rating Anxiety Scale, Self-Rating Depression Scale, and Self-Management Scale for Kidney Transplant Recipients were used. Correlation analysis was used to fi nd factors related to endogenous creatinine clearance, while multiple linear regression was used to identify factors in fl uencing endogenous creatinine clearance. Patients with or without anxiety and depression were divided into groups, and the indexes of the groups were compared using the independent samples t test or chi-squared test.
- 42. Contd,, Results: Anxiety was present in 12.5% of patients, depression in 25%, and a moderate level of self-management of renal transplant recipients had endogenous creatinine clearance within the normal range, and 34.1% had a body mass index not in the normal range .The endogenous creatinine clearance rate was negatively correlated with age and degree of depression, and positively correlated with body mass index, treatment management score, and psychosocial management score. The main in fl uencing factors of endogenous creatinine clearance rate were age, sex, depression, body mass index, and treatment management score. The endogenous creatinine clearance rate and psychosocial management ability were signi fi cantly higher in patients without anxiety and depression than in patients with anxiety and depression. Conclusions: Anxiety and depression showed signi fi cant negative e ff ects on the psychosocial self-management ability and endogenous creatinine clearance rate of renal transplant recipients and thus should be given more attention.
- 43. SUMMARY In today’s seminar we have discussed about the nursing management of patient undergoing renal transplantation including definition, history, indication, pre operative screening and checklist ,contraindication and its management.
- 44. CONCLUSION The kidneys are a vital organ critical to the human body. From filtering waste from blood to produce red blood cells, it serves a crucial role. Renal failure is a serious condition that could complicate the course of many of patients. Therefore, renal transplant is an important aspect leading to the saving the life of individual at end stage. Successful renal transplantation significantly improves the outcome of a patient with end stage renal disease.
- 45. REFERANCE 1)Brunner and Suddarth; Textbook of Medical Surgical Nursing 13th Edition Volume II. New Delhi; Wolters Kluwer Publication. 2)Lewis. Medical Surgical Nursing Assessment and Management of clinical problems.2015. New Delhi. Elsevier. 2nd Edition. Volume II. 3)Petrica A. Potter; Fundamentals of Nursing South Asian Edition Volume I. New Delhi; Elsevier Publications 4)Joyce M. Black, Jane Hokanson Hawks. Medical Surgical Nursing Clinical Management of Positive Outcomes.2015. New Delhi. Reed Elsevier India Private Limited. Volume II.