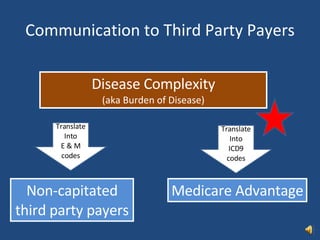
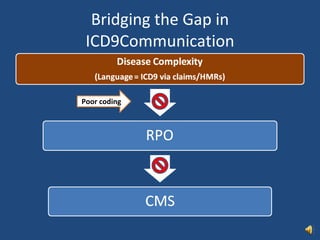
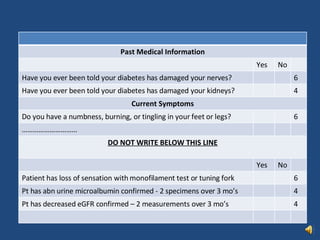
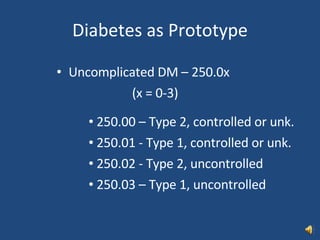
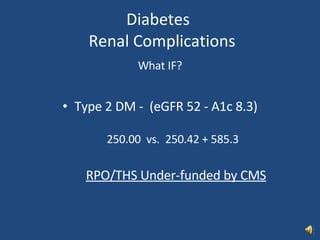
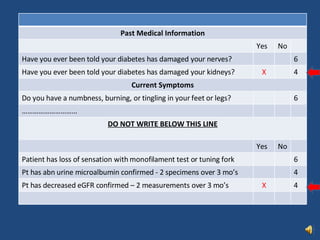
The document discusses strategies for improving ICD-9 coding accuracy and completeness, with a focus on common chronic conditions like diabetes, hypertension, heart disease, and kidney disease. It provides diagnostic criteria and recommended ICD-9 codes for documenting complications from these conditions, such as neuropathy, retinopathy, kidney damage, and congestive heart failure. Checklists and electronic medical record tools are presented as ways to systematically capture this clinical information and apply the proper ICD-9 codes.























































































![Nuevasguiasdislipidemia2018 [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/nuevasguiasdislipidemia2018autoguardado-190507175428-thumbnail.jpg?width=640&height=640&fit=bounds)















































































