
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Bilateral Femur Head Osteonecrosis Diagnosis and Management
Similar to Bilateral Femur Head Osteonecrosis Diagnosis and Management (20)
More from Gashaye Tagele
More from Gashaye Tagele (6)
Recently uploaded
Recently uploaded (20)
Bilateral Femur Head Osteonecrosis Diagnosis and Management
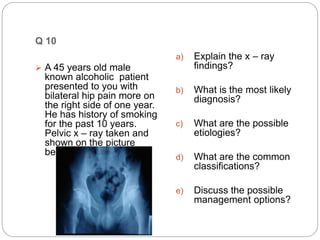
- 1. Q 10 A 45 years old male known alcoholic patient presented to you with bilateral hip pain more on the right side of one year. He has history of smoking for the past 10 years. Pelvic x – ray taken and shown on the picture below a) Explain the x – ray findings? b) What is the most likely diagnosis? c) What are the possible etiologies? d) What are the common classifications? e) Discuss the possible management options?
- 2. Explain the x – ray findings? Ap x ray of pelvis Irregular femur head with sclorosis and lucency with in the head
- 3. What is the most likely diagnosis? Bilateral femur head osteonecrosis
- 4. What are the possible etiologies? traumatic chronic corticosteroid therapy alcoholism Smoking SLE Hyperlipidaemias HIV Hemoglobinopathy CRF DM pregnancy-related
- 8. Discuss the possible management options? Non operative Operative Non operative RWB Decrease activity Medical therapy Osteoporotic drug Cholesterol decreasing agent Steroid…. New way PEMF….considered ECSW….considered Hyperbaric oxygen therapy
- 9. Core Decompression for Ficat stages I and IIA small central lesions in young, non obese patients who are not taking steroids. Bone Morphogenic Proteins Bone marrow mesenchymal cell grafting BONE GRAFT Structural Non structual Tantalum rod
- 10. Porous tantalum rod insertion A novel approach in the treatment of stage I & II precollapse osteonecrosis rod functions analogously to a Cortical Strut Graft allowing structural & osteoconductive properties
- 11. Various Nonvascularized & Vascularized Bone Grafting Procedures Grafting through lateral core track Grafting through femoral neck window- light bulb window Grafting through articular surface window -trap door technique NON VASCULARIZED Iliac crest VASCLARIZED FREE FIBULAR MUSCLE PEDICLE BONE
- 14. Osteotomy Procedures Total Hip Arthroplasty Hip Resurfacing Procedures Stage iii and above More than 30% involvement
- 15. valgus-extension intertrochanteric osteotomy combined with curettage of the avascular segment and autogenous bone grafting was reported to have an 87% success rate at 65 months.
- 16. A transtrochanteric rotational osteotomy of the femoral head reposition the necrotic anterosuperior part of the femoral head to a non–weight-bearing locale. Femoral head and neck segment is rotated anteriorly around its longitudinal axis so that the weight-bearing force is transmitted to what was previously the posterior articular surface o
- 17. Q11.A 34 years old patient presented to your clinic eight weeks post injury complaining of pain over her wrist. X – ray of the wrist is shown below a) What do you see? b) What are the x ray views ued to diagnose this fracture? c) What are the poor prognostic factors for nonunion? d) How would you manage this patient? e) What are the indications for internal fixation of these fractures? f) What approach would you use?
- 18. What do you see? PA x ray view of wrist fracture of scaphoid at the level of waist Displaced No sclorosis or cyst formaed
- 19. What are the x ray views ued to diagnose this fracture? Lateral Scaphoid view Oblique view Supinated Pronated Ziter view/banana view
- 20. What are the poor prognostic factors for nonunion? Displacemennt Proximal delayed Fracture dislocation DSCI Scapholuniate angle>60 deg UNSTABLE FRACTURE
- 21. How would you manage this patient? CT AND MRI Articular surface Open reduction with bone graft Cast Short arm …scaphoid cast Time depending fracture type 4wk to 4month
- 22. What are the indications for internal fixation of these fractures? Any fracture in young medical fit with sign of instablity
- 23. What approach would you use? Open vs percutaneous Volar vs dorsal Headless canulated screw With or with out graft
- 24. Q12 A 32 year old Rt handed female housewife sustained FDA with outstretched hand and injured her right wrist area. She arrived at the EOPD with swollen and painful Rt wrist. distal neurovascular exam is intact. Xray is attached below.
- 25. What is the most likely diagnosis? What additional injuries are you most concerned about? Distal radial fracture – colls type Distal radio ulnar joint TFCC
- 26. What is the most appropriate initial treatment for this patient? ATLS Analgesic Proper evaluation Closed reduction with bier block or hematoma block And splinting
- 27. When do you consider operative treatment in this patient? displaced intra-articular fx volar or dorsal comminution articular margins fxs severe osteoporosis dorsal angulation >5° or >20° of contralateral distal radius >5mm radial shortening comminuted and displaced extra-articular fxs (Smith's fx) progressive loss of volar tilt and loss of radial length following closed reduction and casting associated ulnar styloid
- 28. What will be your operative plan for this patient? Joint spaning ex fix CT scan AUGMENT WITH ORIF VOLAR PLATE PERCUTANEOUS PIN
- 31. What potential complications could this women will suffer ? OA stiffness CTS Malunion Tendon irritation
- 32. Reference Rockwood and Green’s Fractures in Adults 8ed. Campbel's 13th ed. Orthobullet
- 33. THANK YOU!
Editor's Notes
- Bone Morphogenic Proteins Bone marrow mesenchymal cell grafting
- Better out come in young<50yr Postraumatic and idiopathic than alcholic or steroid use