1. Arch Neuropsychiatry 2019;56:302−310
https://doi.org/10.29399/npa.23369
302
REVIEW
Effect of Exercise on Major Depressive Disorder and
Schizophrenia: A BDNF
Focused Approach
Evrim GÖKÇE , Emel GÜNEŞ , Erhan NALÇACI
Department of Physiology, Ankara University, Faculty of
Medicine, Ankara, Turkey
Psychiatric disorders are remarkable health problems that cause
a
massive social and economic burden, and the issue of their
long-term
and effective treatment is subjected to discussion. The effect of
physical
activity and exercise is under investigation in the treatment of
the major
depressive disorder (MDD) and schizophrenia which are
accompanied by
cognitive dysfunctions. Scientists focus on the positive effects
of exercise
on learning, memory and attention parameters while
investigating the
regulatory role of brain-derived neurotrophic factor (BDNF). In
this
2. review, the effect of aerobic exercise on peripheral BDNF
levels in MDD
and schizophrenia is examined by including human studies in
which
acute and chronic aerobic exercise are applied. The results
showed that
aerobic exercise caused different responses on BDNF levels,
and some
of the studies were accompanied by the improvement in
cognitive
functions in BDNF changes. In order to comprehend the effect
of aerobic
exercise in MDD and schizophrenia, it is understood that
applying
studies on larger and paired participant groups with different
exercise
frequencies and tensions in necessary.
Keywords: Brain derived neurotrophic factor, aerobic exercise,
schizophrenia, major depressive disorder, cognitive functions
ABSTRACT
Cite this article as: Gökçe E, Güneş E, Nalçacı E. Effect of
Exercise on Major Depressive Disorder and Schizophrenia: A
BDNF Focused Approach. Arch Neuropsychiatry
2019;56:302-310.
302
Correspondence Address: Emel GÜNEŞ, Ankara Üniversitesi
Tıp Fakültesi, Fizyoloji Anabilim Dalı, Ankara, Turkey • E-
mail: [email protected]
Received: 04.09.2018, Accepted: 27.03.2019, Available Online
Date: 15.10.2019
4. BDNF
BDNF, secreted from both the central nervous system and
peripheral
tissues, is a protein of the neurotrophin family, including the
nerve growth
factor, neurotrophin-3 and neurotrophin-4/5. This structure,
which is
synthesized in the form of pre-pro-BDNF in the endoplasmic
reticulum
and which moves to the trans-golgi network through the Golgi
body, is
secreted as mature BDNF or pro-BDNF and is stored in platelets
at a high
level (4). BDNF, with the sources of neurons, microglia and
astrocytes in
the brain, are also secreted from vascular endothelium,
lymphocytes and
smooth/striated muscles. Tropomyosin receptor kinase B
(TrkB), one of
the BDNF receptors, binds to the mature BDNF while p75 (low-
affinity
nerve growth factor receptor) binds to pro-BDNF.
BDNF was first isolated from the tissue of pig brains in 1982
and detected
in human blood in 1995. It has been reported to cross the blood-
brain
barrier and the serum and plasma levels of BDNF have been
associated
with age, gender, and body mass index (5). BDNF is a protein
that affects
neuronal survival, neurogenesis and neuroplasticity in the
central nervous
system and play a role in cell differentiation, axon and dendrite
growth,
5. synapse formation and synaptic plasticity, and its expression
and release
are related to neuronal activity. BDNF is critical for synaptic
formation
in dopaminergic, glutamatergic and serotonergic neuronal
conduction
and cognitive processes. The main effect of BDNF is on
synaptic
function and neuronal morphology in a region-specific manner
(6). It is
responsible for short-term memory and long-term memory
potentiation
and performs tasks related to remembering, cognition,
emotional state,
spatial direction, and learning (7). BDNF messenger RNA
(mRNA) has
been widely observed in the hippocampus and cerebral cortex.
BDNF-
containing vesicles are found in both the axonal terminals and
dendrites,
and BDNF is also secreted from astrocytes (8). BDNF secretion
may be
via Ca2+ influx from the postsynaptic or presynaptic area Ca2+
influx or
Ca2+ release from intracellular stores (9). Studies reporting the
cognitive
benefits of exercise suggest that BDNF is involved in this
mechanism (10,
11). Animal studies showed that BDNF and tropomyosin
receptor kinase
B (TrkB) receptor activation was increased in various brain
regions during
and after exercise, while human studies detected peripheral
BDNF in the
serum and plasma and found a relationship between the cerebral
and
6. INTRODUCTION
https://orcid.org/0000-0003-1548-8785
https://orcid.org/0000-0003-3599-5151
https://orcid.org/0000-0003-4850-4745
Gökçe et al. Exercise, BDNF and CognitionArch
Neuropsychiatry 2019;56:302−310
303
peripheral BDNF levels, which varied according to the type,
duration and
frequency of exercise in different studies (12–14).
Exercise, BDNF and Cognition
Meta-analytical reviews indicate that acute and chronic aerobic
exercise
has a developmental effect on cognition with the most dramatic
effect seen
on its executive functions (15). In this area, where the
mechanism of action
is not fully elucidated, BDNF is suggested to have a potential
mechanism.
The BDNF response to aerobic exercise has been investigated in
the
literature in relation to different acute and chronic exercise
programs at
different doses. In addition to aerobic exercise-induced BDNF
responses,
these studies have also examined cognitive performance
findings. The
method generally used in the studies examining the effects of
aerobic
7. exercise on BDNF and cognition is the measurement of the
BDNF level
before and after exercise and the application of cognitive tests.
The effect
of BDNF on cognition has been explored mainly through
memory tasks.
The definition of the hippocampus as the main site for BDNF
expression
in the brain (16) its effect on memory tasks makes this choice
meaningful.
Although human studies offer limited opportunities to monitor
BDNF
levels in the brain, it has been found that the peripheral BDNF
levels,
hippocampal volume, and spatial memory results are correlated
(17).
Effect of Exercise on BDNF and Cognitive Function in Healthy
Individuals
Meta-analytical reviews examining the effect of acute exercise
on
peripheral BDNF (18) reported contradictory results, but
predominantly
indicated an increase in BDNF and agreed that this increase was
transient. On the other hand, due to the different methods used
in these
studies, it is established that the responses detected were not
completely
consistent. After 30 minutes of acute exercise, an increase was
observed
in the cognitive functions and BDNF levels of healthy subjects
evaluated
by the Face Recognition Test and the Stroop Test, but the
relationship
between the two parameters was not evaluated (19).
8. In a review suggesting a positive relationship between exercise
severity
and peripheral BDNF levels, it was reported that high-intensity
acute
exercise provided the greatest increase in BDNF in healthy
subjects. On
the other hand, the BDNF level returned to baseline between 10
and 60
minutes (18). After 20 minutes of intense exercise, healthy
individuals
showed improvement in cognitive findings and BDNF levels
assessed by
the visual spatial perception test, and a significant relationship
was found
between motor memory and BDNF data (20).
In a study evaluating cognitive performance by the reaction
time in the
Visual Spatial Attention Test and EEG after 30 minutes of
moderate acute
exercise in non-trained individuals, the BDNF levels increased
and the
reaction time decreased in exercise groups. The neuroelectric
signals,
which were interpreted as increased attention in EEG (P3
amplitude) and
readiness to respond to stimulus (CNV amplitude), were only
increased
in trained individuals. A significant relationship between BDNF
and
cognitive performance levels was not found. The researchers
interpreted
their results as cardiovascular fitness being involved in the
mechanism of
action of exercise on cognition (21).
9. A study conducted with healthy subjects that performed severe
acute
aerobic exercise evaluated the BDNF level, inhibitory control
using the
Stroop Test, and cognitive flexibility using Part B of the Trail-
Making Test,
and reported increased cognitive success findings and BDNF
levels. A
significant relationship was found between the increased BDNF
level
and cognitive flexibility success findings. The authors
suggested that
improvement in cognitive performance related to the prefrontal
area in
response to acute exercise could be attributed to an increase in
the BDNF
level (10).
In another study conducted in healthy individuals, the BDNF
level and
executive functions were evaluated using the Wisconsin Card
Sorting
Test before and after high-intensity intermittent exercise, and
while the
plasma BDNF level did not change, the serum BDNF level
increased.
According to the results of the Wisconsin Card Sorting Test, the
number
of categories completed and the number of correct responses
increased,
and the number of total and recurrent errors decreased. The
authors
did not find a significant relationship between BDNF
concentration
and the results of executive functions related to the prefrontal
cortex;
10. however, they commented that cognitive performance responded
more
to the increased intensity of exercise (22). It was also reported
that
the increase in BDNF after acute aerobic exercise was
associated with
exercise duration. The increase in BDNF was significantly
higher than in
exercise lasting longer than 30 minutes compared to exercise for
less than
30 minutes. This can be interpreted as different exercise times
affecting
brain functions differently. In a study on acute exercise and its
effect on
cognitive functions, it was shown that cognitive benefit
emerged only
through exercise lasting longer than 20 minutes (23). Other
studies
suggested that the duration and intensity of exercise produced
the best
result related to moderate exercise, and therefore the effect of
regular
exercise on BDNF and cognition was more dramatic (18, 24).
Regular
exercise increases the BDNF level in the hippocampus and
improves
learning and memory processes.
Chronic exercise in children and young adults improved
working
memory, selective attention, and inhibitory control findings
(25). In a
six-month aerobic exercise study conducted with elderly men,
the gray
matter volume increased and the peripheral BDNF increased in
the
11. prefrontal and cingulate cortex areas associated with increased
physical
activity (26).
Effect of Exercise on BDNF and Cognitive Function in Major
Depressive Disorder (MDD) and Schizophrenia
MDD, which is one of the leading causes of global disease
burden,
manifests with cognitive and somatic symptoms. In recent years,
BDNF
has been used as a biomarker in psychiatric disorders, such as
MDD,
schizophrenia and bipolar disorder, and the BDNF level has
been shown
to be lower in patient groups than in healthy individuals (27–
29). It
was suggested that the BDNF level is lower in MDD cases, and
a higher
level BDNF is associated with less depressive symptoms and
improved
cognitive functions compared to the healthy population (30, 31).
In
case studies, granular neuron loss, reduced hippocampal
volume, and
regressed peripheral level of BDNF and BDNF mRNA
expression in
lymphocytes were reported (32), and suicidal behavior was
associated
with a low peripheral/cerebral BDNF level (in the hippocampus
and
prefrontal cortex) (33). It was found that the peripheral level of
BDNF
could be used to predict the response to antidepressant
treatment in
MDD, and there was an increase in this level in response to
drug therapy;
12. however, the results regarding the relationship between
improvement in
mood and BDNF increase were contradictory (34).
It is not yet clear whether the clinical manifestation of the
BDNF variant
Val66Met is a risk factor for MDD. However, in a review, it
was proposed that
this variant reduced the response to drug treatment (35).
Schizophrenia,
on the other hand, is a severe mental disorder characterized by
psychosis
and generally presents with cognitive dysfunctions related to
problem
solving, memory, and executive functions (36). Animal models
have
drawn attention to the role of BDNF in the development and
activation
of psychosis-related neurotransmitters. It is stated that the
changes in
the BDNF level may contribute to neuroplasticity disorder
during brain
development and synaptic connection disorders, and the
morphological,
neurochemical and cell architecture anomalies observed in the
brain in
schizophrenia (37). It is well known that in schizophrenia,
neurocognitive
losses are observed in memory, attention, processing speed, and
executive
Gökçe et al. Exercise, BDNF and Cognition Arch
Neuropsychiatry 2019;56:302−310
13. 304
functions. A meta-analytical review of 16 studies reported that
patients
with schizophrenia had significantly lower peripheral BDNF
(27), with
memory disturbances and smaller hippocampal volume findings
being
associated with a reduced BDNF level (38). In untreated
psychosis, the
serum BDNF level was shown to be low and correlated with the
duration
of psychosis, and drug-induced psychosis models indicated a
relationship
between a reduced BDNF mRNA concentration and psychotic
symptoms
(39). The visual spatial memory performance and attention were
found to
be poor in schizophrenia patients with the BDNF Val66Met
variant, and
a low BDNF level was observed to be correlated with reduced
cognitive
functions (40).
MATERIAL AND METHODS
For this review, human studies published in English were cross-
searched
on the PubMed and Web of Science search engines using the
keywords
BDNF-exercise-cognition-major depressive
disorder/schizophrenia and
BDNF-exercise-major depressive disorder/schizophrenia and
those that
only included aerobic exercise were selected. Two studies
examined the
effect of aerobic exercise on cognition and BDNF in
14. schizophrenia, three
examined the effect of aerobic exercise on cognition and BDNF
in MDD,
and seven studies examined the effect of aerobic exercise on
BDNF in
MDD. Three of the studies used acute and nine used chronic
aerobic
exercise as a method. The total number of participants in 12
studies was
385. In MDD and schizophrenia, the responses of peripheral
BDNF to
exercise, the relationship between exercise and cognitive
performance
findings, and the underlying mechanism of these responses were
discussed, and how BDNF and cognitive functions changed with
aerobic
exercise was examined.
RESULTS
The findings suggest that aerobic exercise increases the
peripheral
BDNF level. No significant increase in BDNF was observed in
three of
the MDD studies, whereas a significant increase in BDNF was
noted
in all the remaining studies. While four studies examining
BDNF and
cognitive performance findings together showed a significant
increase
in both parameters, the improvement in cognitive performance
was not
accompanied by an increase in BDNF in one of the studies.
DISCUSSION
Effects of Exercise in MDD
It is reported that 5% of the global population has been
15. diagnosed with
MDD and 1% with schizophrenia, and 20-30% of all of these
patients are
resistant to treatment (41– 43). It is known that in MDD, the
workload
capacity of individuals is reduced by 80 to 90% compared to
their healthy
counterparts, and physical activity is decreased in schizophrenia
and is
accompanied by cognitive disorders (44, 45).
Studies have shown that neuronal activity affects the synthesis,
secretion
and signaling of neurotrophin, which has an impact on the
postsynaptic
response, synaptic morphology, presynaptic transmitter
secretion, and
membrane excitability.
In nine of the 12 studies we reviewed, an increase in BDNF was
reported
in the period following aerobic exercise (46–54). These data
seem to
agree with the premise that exercise contributes to the
promotion and
maintenance of neuron functions through a mechanism mediated
by neurotrophins. It has been suggested that one of the
mechanisms
Table 1. Summary of studies investigating the effect of aerobic
exercise on BDNF and cognitive functions in schizophrenia and
major depressive disorder.
Researcher
Participants
16. (Exercise/Control)
Exercise modelity Cognitive effect BDNF response
Kimhy et al., 2015* 13/13
12 weeks, 3 times per week,
60 minutes
In exercise group global cognitive
performance↑
In exercise group
%11, in standard
treatment group %1,9 ↑
Nuechterlein et al., 2016* 7/9
10 weeks, 4 times per week,
30-45 minutes
In exercise group social cognition, working
memory, processing speed, attention-
vigilance performance ↑
In exercise group ↑
Gourgouvellis et al., 2018 ** 8/8
8 weeks, 3 times per week,
60 minutes
In exercise group global cognition,
recognition memory, visual learning and
memory performance ↑
17. In exercise group ↑
Vedovelli, 2017** 22/10
12 weeks, 3 times per week,
60 minutes
In exercise group processing speed,
executive function, attention, working
memory, işlemleme hızı, recall, response
inhibiton ↑
In exercise group ↑
Krogh et al., 2014** 41/38
12 weeks, 3 times per week,
45 minutes/streching
In aerobic exercise group verbal memory
performance ↑
No significant change
Kallies et al., 2018** 30/-
Acute aerobic exercise, not
specified frequency/duration
- ↑
Kerling et al., 2017 ** 22/-
6 weeks, 3 times per week,
45 minutes
- No significant change
18. Salehi et al., 2016** 20/-
4 weeks, 3 times per week,
40-45 minutes
- ↑
Schuch et al., 2014** 15/11
3 weeks, 3 times per week, not
specified duration
- In exercise group ↑
Toups et al., 2011**
70/- 12 weeks, not specified
frequency
- No significant change
Meyer et al., 2016** 24/-
Acute aerobic exercise,
30 minutes
- ↑
Meyer et al., 2016** 24/-
Acute aerobic exercise,
30 minutes
- ↑
*Schizophrenia studies
**MDD studies
Gökçe et al. Exercise, BDNF and CognitionArch
19. Neuropsychiatry 2019;56:302−310
305
responsible for increased BDNF may be the increase in the
cerebral
blood flow. Another proposition is that exercise-related increase
in the
insulin-like growth factor (IGF)-1 and norepinephrine levels
may increase
the expression of BDNF mRNA. It has also been argued that
decreased
blood volume due to water loss may increase the BDNF
concentration.
BDNF plays several important roles in synaptic plasticity and
affects
different aspects of synaptic transmission. In the central
nervous
system, BDNF can increase the number of excitatory and
inhibitory
synapses by regulating axonal morphology or directly
improving
synapse formation (6). Furthermore, it enhances the maturation
and
stabilization of neurotransmitter secretion at the cellular and
molecular
level, which increases the number of functional synapses. It
regulates
the increase in proteins involved in neurogenesis, learning and
memory,
and neuronal survival, including those regulating the protein
quality
control, mitochondrial biogenesis, and the resistance of cells to
oxidative,
metabolic and proteotoxic stress. In the literature, it has been
20. reported
that BDNF secreted from the cerebral endothelium following
acute
aerobic exercise was responsible for the effect of exercise on
cognition
(55). This function of BDNF appears to be consistent with the
memory
responses obtained from studies that included the findings of
cognitive
function in this review.
The mechanism of action of BDNF on neuroplasticity is claimed
to be
through increasing the calcium mRNA, cAMP response binding
protein
(CREB), and synapse I level (56). Exercise can produce
persistent increases
in phosphorylated CREB and BDNF levels that continue
throughout the
exercise period. An exercise-induced increase in BDNF levels
increases
the expression of key presynaptic molecules associated with
synaptic
transmission, such as synapse I and synaptophysin with a
vesicular
function at the presynaptic nerve terminals. Especially in
glutamatergic
synapses, BDNF plays a key role in initiating signal
transduction with
the TrkB and p75 receptors in regulating activity-dependent
synaptic
structure and function. Mature BDNF primarily stimulates the
TrkB
receptor, while proBDNF targets the p75 receptor. Mature
BDNF binds to
the extracellular domain of receptor TrkB and activates
21. phosphorylated
TrkB, phosphotidylinositol-3 kinase (PI3K), mitogen-activated
protein
kinase (MAPK), phospholipase-Cγ (PLCγ) and guanosine
triphosphate
(GTPase) pathways. The PI3K pathway showing an
antiapoptotic effect
modulates the synaptic plasticity of N-methyl-D-aspartate
(NMDA)
receptors and increases dendritic growth and branching (Figure
1) (57).
The PLCγ pathway is responsible for increased CaMKII and
CREB activation
through the secretion of intracellular Ca2+. The MAPK signal is
required
for the activation of the extracellular signal-regulated kinase 1
and CREB.
This pathway is important for the synthesis of the cytoskeleton
protein,
as well as dendritic growth and branching in hippocampal
neurons. The
activation of the GTPase pathway stimulates the synthesis of
actin and
microtubules, resulting in the growth of neuronal fibers (58).
The BDNF
responses seen in the reviewed studies on chronic aerobic
exercise may
be related to increased CREB phosphorylation of the repetitive
stimulus,
leading to prolonged structural and functional changes in
synapses. It is
reported that the CREB function in activity-dependent long-
term neuronal
plasticity is a necessary molecule for long-term memory
formation. It has
22. been reported that by increasing the presence and activity of
CaMKII
and BDNF levels and reducing calcineurin phosphatase levels,
exercise
boosts the synthesis of important signaling molecules that are
critical for
learning and memory (59).
In their study with MDD cases, Gourgouvellis et al. observed an
increase in the BDNF level and visual learning, memory and
recognition
memory performance following cognitive behavioral therapy
and
aerobic exercise (48). In accordance with these results, in the
literature,
increased BDNF and CREB mRNA levels were associated with
exercise
in mice, and the highest BDNF expression was associated with
the
highest CREB expression and spatial memory ability (60). In
another
study, it was found that exercise increased the active CREB
form,
and the learning ability of mice was also significantly increased
after
exercise, and the highest elevation in the BDNF level belonged
to those
that learned fastest (61).
The acute aerobic exercise studies included in this review (53,
54) also
reported elevated BDNF levels. Considering the studies that did
not
report an increase in BDNF in response to chronic aerobic
exercise, it
23. can be regarded that transient BDNF elevations are responsible
for the
chronic benefits of exercise in MDD. It could be the case that
exercise has
a curative effect through transient elevations in BDNF without
long-term
changes in basal BDNF, which leads to long-term
neurophysiological
changes. The clinical effectiveness of exercise in curing MDD
may also
result from its favorable effects on monoaminergic function,
neurogenesis,
and immunity. Exercise causes changes in markers associated
with the
monoamine metabolism, including monoamine, monoamine
receptors,
and carriers, and among these changes are the activation of
serotonergic
neurons in the dorsal raphe nucleus (DRN) by low-intensity
exercise. It
has been suggested that the effect of exercise on serotonergic
activity
can explain its curative effect on depressive symptoms. The
central
serotonergic system is built into the DRN and has projections
over
large areas of the brain. It is considered that exercise
demonstrates
its antidepressant effect through the serotonergic neurons in
DRN.
Accordingly, increased serotonin synthesis, metabolism, and
secretion
are observed during and after exercise. It has been shown that
exercise
has the effects of inducing hippocampal BDNF expression by
increasing
24. the NE/5-HT levels of antidepressants. This has led to the
hypothesis
that increased BDNF mRNA expression associated with exercise
may be initiated by monoaminergic activation. Studies indicate
that
noradrenaline-mediated signaling may be particularly important
in the
modulation of the BDNF gene expression through exercise.
These results
confirm that noradrenaline stimulation is an important initial
event in
cellular mechanisms, leading to improved BDNF transcription
following
physical exercise. Together with antidepressants, exercise is
thought to
have a similar effect on the induction of noradrenaline
activation and
increase in BDNF via β-adrenergic receptors (Figure 2) (62).
Evidence from human and animal studies has shown that
monoaminergic
hypofunction is a curable component of depression (63).
Therefore,
antidepressant drugs have been developed to increase
serotonergic (5-
Figure 1. Binding of mature BDNF to receptor TrkB activates
PI3K, MAPK, PLCγ and GTP-
less pathways.
Gökçe et al. Exercise, BDNF and Cognition Arch
Neuropsychiatry 2019;56:302−310
306
25. However, three of the reviewed studies showed that aerobic
exercise did
not cause an increase in BDNF in cases with MDD (69–71).
Consistent
with these results, a meta-analysis in the literature reported that
chronic
aerobic exercise did not affect the BDNF level in MDD and
suggested that
the predominance of female patients in the sample included in
the study
might have led to this finding (72). The authors reported that
the cerebral
blood flow, blood volume, and other circulating
neurotransmitters
might be the cause of the exercise-triggered changes in neuronal
life, synaptogenesis, and neural circuitry. In another chronic
aerobic
exercise study conducted with healthy individuals by the same
group of
researchers, the findings indicated a rapid increase in the BDNF
level in
men following exercise, but no changes were observed in
women (73).
Effects of Exercise in Schizophrenia
BDNF, which increases the expression of dopamine receptors in
the
brain by mimicking the effect of antipsychotic drugs, is
reported to
regress manic mood (74, 75). Similarly, schizophrenia studies
have
shown that exercise improves cognitive abilities and physical
health (2,
76) and that low-level BDNF is associated with negative
symptoms and
26. may contribute to the psychopathology of the disease (77).
Since BDNF is widely distributed throughout the central
nervous system
and plays a role in various psychiatric disorders, impairment in
BDNF
signaling is not specific to schizophrenia. However, considering
the
effect of BDNF on the plasticity and neuronal viability of
dopaminergic,
serotonergic, and cholinergic neurons, and the importance of all
these
pathways in the pathophysiology of schizophrenia, it can be
concluded
that BDNF can be a useful biological marker for the clinical
status and/
or prognosis of people with this disease.
In the schizophrenia studies included in this review (46, 47), the
increase
in the peripheral BDNF level and the improved cognitive
performance
findings in response to exercise support the idea that exercise
can
enhance neurotrophic and neuroprotective mechanisms, and thus
leading to an improvement in the symptoms of schizophrenia.
One of
the possible ways in which aerobic exercise improves the
symptoms
of schizophrenia is that it enhances drug efficacy by affecting
the
pharmacokinetics of antipsychotics, for example, by changing
drug
distribution and reducing drug excretion (78).
BDNF is a neurotrophin that is not only related to neuronal
27. protection
and development but also effective in synaptic regulation,
learning, and
memory. Since BDNF plays an important role in regulating
synaptic
plasticity, schizophrenia deficits can be understood in the
context of
learning and the molecular and cellular mechanisms of memory.
Concerning the pathogenesis of schizophrenia, particularly
neurodevelopmental and neurotoxicity-related factors,
neurotrophins,
such as BDNF can provide an explanatory framework at
molecular
and cellular levels. The synaptic changes that occur due to
problems in
BDNF expression can alter neurotransmitter pathways that are
classically
involved in the pathophysiology of schizophrenia; e.g.,
dopaminergic
and gamma-aminobutyric acid (GABA) systems (79, 80).
Abnormal
BDNF and TrkB mRNA expression in the hippocampus of
individuals
with schizophrenia and mood disorders showed that the main
features
of hippocampal signal transmission and plasticity can be
affected in
these major mental disorders (81).
In patients with schizophrenia, a deficiency in BDNF signaling
mediated by receptor TrkB can result in decreased GABA
synthesis in
the dorsolateral prefrontal cortex. This may lead to a change in
the
perisomatic inhibition of pyramidal neurons by decreasing the
28. gamma
neuron activity at synchronized frequencies required for
working
memory. Consistent with the literature, Nuechterlain et al. (47)
showed
Figure 2. Relationship between BDNF and glutamate receptors.
HT) or noradrenergic (NE) neurotransmission to eliminate the
effects of
depression.
Seven studies (48–54) in this review reported that aerobic
exercise in
MDD increased BDNF, and two demonstrated that elevated
BDNF was
accompanied by improved cognitive functions (48, 49). In the
literature,
the reduced levels of neurotrophic factors and neurogenesis
have been
suggested to contribute to the neurotrophic hypothesis of
depression
(64). It is recommended that antidepressants increase BDNF
expression,
and in turn, BDNF increases the effect of antidepressants using
a similar
neurochemical pathway (65). Considering that neurotrophic
factors,
especially BDNF, can contribute to the treatment of depression,
exercise
can be used as a therapeutic tool.
It is reported that skeletal muscle secretes cytokine in response
to exercise
and increases interleukin (IL)-6, which then crosses the blood-
brain
29. barrier and triggers BDNF secretion from platelets. BDNF
expression in
the central nervous system has been found to be strongly
associated with
the IL-6 level and platelet count (66). During acute exercise, the
increase
in IL-6 produced by the working muscles inhibits tumor
necrosis factor α
(TNF-α) and IL-1β expression. Therefore, it is possible that the
therapeutic
effect of exercise on depressive symptoms may prevent
proinflammatory
etiology through changes in immune functions.
The peroxisome proliferator-activated receptor-gamma
coactivator
(PGC)-1α also appears to play a role in facilitating the effects
of exercise
on brain health and is part of the mechanism by which exercise
induces
hippocampal BDNF expression. Exercise first induces the
expression of
the estrogen-related receptor (ERR) α gene in the brain, then
stimulates
PGC-1α expression. The increased activity of the ERRα/PGC-1α
complex
through exercise induces the expression of the BDNF gene (67).
One of
the reviewed studies, exercise was reported to have a protective
effect
against depression by altering the metabolism of the kynurenine
(68).
The activation of PGC-1α increases the skeletal muscle
expression of
the aminotransferases of kynurenine, protecting the brain from
stress-
30. related changes through the conversion of kynurenine to
kynurenic acid,
a metabolite that cannot cross the blood-brain barrier, and
reducing
plasma kynurenine. These studies indicate that PGC-1α in the
muscle and
brain can mediate the effects of exercise on cognitive functions.
Gökçe et al. Exercise, BDNF and CognitionArch
Neuropsychiatry 2019;56:302−310
307
that aerobic exercise increased the peripheral BDNF level in
patients
with schizophrenia and improved working memory findings.
In negative symptoms of schizophrenia, the mechanism of
glutamate
dysfunction was implicated, and increased glutamate function
was
shown to have the potential to reduce such symptoms (82).
BDNF can
directly alter glutamate signaling by altering the expression of
glutamate
receptor subunits and Ca2+ regulatory proteins. It can also have
an impact
on glutamate signaling by inducing antioxidant enzyme
production,
energy regulating proteins, and the members of the
antiapoptotic Bcl2
family. Glutamate stimulates BDNF production, which, in turn,
affects
neuronal glutamate sensitivity, Ca2+ homeostasis, and plasticity
31. (83). In the
early studies examining the relationship between glutamatergic
system
and BDNF, mature BDNF was reported to induce the rapid
effects of
glutamate secretion and the short- and long-term effects of post-
synaptic
responses to neurotransmitters. A study focusing on the acute
effect of
BDNF on the hippocampus neurons of rats found that
glutamatergic
synaptic transmission was increased in 30% of the cells, but this
increase
was not seen when receptor TrkB was inhibited (84). This data
suggests
that presynaptic modification is effective in increasing
glutamatergic
synaptic transmission, and BDNF is involved in this
modulation. Although
the studies included in this review did not examine the state of
negative
symptoms in schizophrenia, the improvement in cognitive
functions
was accompanied by elevated BDNF. This improved clinical
state can be
explained by aerobic exercise increasing the use of glutamate by
the brain.
A decreased serum BDNF level has been shown to correlate
with
processing speed, attention, executive functions, and poor
performance
in working memory, and the relationship between serum BDNF
and
cognitive test performance has been emphasized. In the
schizophrenia
32. studies included in this review, the increase in the BDNF level
through
exercise accompanied by improvement in cognitive functions
seems to
be consistent with the literature (85, 86). Exercise may be
involved in this
process through exercise-induced neuronal activity, and it can
change
cognitive performance findings. Similarly, considering that
physical
health deterioration associated with the lack of physical activity
in
schizophrenia reduces the average life expectancy by 10 to 15
years due
to suicide, it is possible to comment that exercise also has an
effect on life
expectancy (87).
Reviewing the Findings on MDD and Schizophrenia Together
Exercise appears to be involved in the development of synaptic
plasticity
in the adult hippocampus through a BDNF-mediated mechanism.
The
major area of BDNF expression in the brain is the
hippocampus. The
findings of the MDD and schizophrenia studies included in this
review
being more significant for memory performance (47–49, 69) can
be
interpreted in this context, and the relatively less effect of
BDNF on the
other cognitive tasks can also be attributed to this. On the other
hand, it
is known that the BDNF level increases with antidepressant
treatment.
In one of the studies included in this review that detected an
33. increase in
BDNF (52), 80% of the participants used one or more
antidepressants.
However, in another study in which the participants used
antidepressants
(71) no increase was detected in BDNF. Therefore, in similar
studies, the
effect of drug interaction should also be taken into
consideration. The
contradictory results in the literature may be due to the effect of
gender
on BDNF responses. It has been reported that gender has an
effect on the
relationship between the BDNF level and general cognitive
functions in
schizophrenia, and this relationship is only observed in women
(88). In this
review, homogeneous groups were not included in the studies
examined,
and the effect of BDNF and cognitive functions were observed
in mixed
groups. In aerobic exercise studies, the duration and intensity of
exercise
can also have an impact on the results. In one study that did not
report
an increase in BDNF, exercise duration was limited to three
weeks, and
no data was provided on exercise intensity. Among the chronic
aerobic
exercise studies included in this review, the longest exercise
intervention
lasted 12 weeks. Longer regular exercise programs can produce
different
findings. It should also be kept in mind that increased BDNF
responses
after exercise may be related to the basal BDNF level of the
34. individual.
In future studies, considering the number and function of
platelets
known to store BDNF can offer new insights. It has been
reported that
the responses of BDNF to exercise in healthy individuals are
affected
by a number of different variables, such as age, gender, exercise
type,
exercise duration, and body mass index (89, 90). Therefore,
examining
the effect of exercise in psychiatric disorders indicates the need
for
more homogeneous study groups. In brief, the psychological
effect of
exercise on cognition is associated with increased autonomic
response,
physical well-being, and increased quality of life, whereas the
mechanism
of action of BDNF in this review is evaluated under the
framework of a
biological basis.
The proposition that BDNF may facilitate improvement in
cognitive
functions in disorders that involve structural changes to the
brain requires
further investigation. The limited number of studies we
reviewed and the
absence of a significant change in the BDNF level in three of
the studies
(69–71) make it difficult to make a comprehensive
generalization on the
subject.
CONCLUSION
35. Although there are studies showing that exercise is protective
for
brain health, affects cognition and mood, and regresses
symptoms
in psychiatric disorders, the number of studies discussing
cognitive
performance and BDNF responses in depression and
schizophrenia
is limited. Despite all these limitations and contradictory
results, there
are more studies showing that exercise provides an increase in
the
BDNF level. Studies examining the cognitive performance
findings have
obtained data revealing the enhancing effect of exercise,
especially on
memory responses. Although it does not diminish the
importance of
traditional therapies, exercise can be considered as a low-cost
supportive
treatment for MDD and schizophrenia. The dynamic nature of
the brain
can allow for a positive effect of exercise as an external factor
on these
disease processes, and support individuals’ functionality in
everyday
life by increasing their ability to adapt. The promotion of
behavioral
approaches, such as exercise can contribute to the improvement
of the
Figure 3. Reciprocal relationship of BDNF, 5-HT, NE
Exercise
BDNF ↑BDNF mRNA ↑
36. Synaptic 5-HT
CREB fosforilation
and BDNF gene
transcription
Anterograde transport and
secretion
Activation of TrkB receptor
NE/5HT synthesis/secretion
Antidepressants (SSRI, SNBI)
Activation of
NE/5-HTRs
Gökçe et al. Exercise, BDNF and Cognition Arch
Neuropsychiatry 2019;56:302−310
308
general health state by increasing the general well-being of the
person, as
well as regressing chronic and treatment-resistant psychiatric
disorders.
By learning more at the molecular level about the pathways
underlying
synaptic plasticity, we can go one step further in finding
protective and
curative ways to ensure brain health, which may also include
37. increasing
BDNF. Further studies planned with larger and homogeneous
participant
groups and different intensity and intensity of exercise will lead
the way
to providing an understanding of the effect of exercise on the
prevention
and treatment of psychiatric disorders.
Peer-review: Externally peer-reviewed.
Author contributions: Concept – EG, EG, EN; Design – EG, EG,
EN; Supervision – EG,
EG, EN; Data Collection &/or Processing – EG, EG, EN;
Analysis&/or Interpretation – EG,
EG, EN; Literature Search – EG, EG, EN; Writing Manuscript–
EG, EG; Critical Review – EN.
Conflict of Interest: No conflict of interest was declared by the
authors.
Financial Disclosure: The authors declared that they did not
receive financial support
for this study.
REFERENCES
1. Zoladz JA, Pilc A. The effect of physical activity on the
brain derived
neurotrophic factor: from animal to human studies. J Physiol
Pharmacol
2010;61:533–41.
2. Firth J, Stubbs B, Rosenbaum S, Vancampfort D, Malchow
B, Schuch F,
Elliott R, Nuechterlein KH, Yung AR. Aerobic Exercise
38. Improves Cognitive
Functioning in People With Schizophrenia: A Systematic
Review and Meta-
Analysis. Schizophr Bull 2017;43:546–556. [CrossRef ]
3. Erickson K, Voss M, Prakash R, Basak C, Szabo A,
Chaddock L, Kim J, Heo S,
Alves H, White S, Wojcicki T, Mailey E, Vieira V, Martin S,
Pence B, Woods J,
McAuley E, Kramer A. Exercise training increases size of
hippocampus and
improves memory. Proc Natl Acad Sci U S A 2011;108;3017–
3022. [CrossRef ]
4. Pliego-Rivero FB, Byatti N, Giannakoulopoulos X, Glover
V, Bradford HF,
Stern G, Sandier M. Brain-derived neurotrophic factor in human
platelets.
Biochem Pharmacol 1997;54:207–209. [CrossRef ]
5. Poduslo JF, Curran GL. Permeability at the blood-brain and
blood-nerve
barriers of the neurotrophic factors: NGF, CNTF, NT-3, BDNF.
Brain Res Mol
Brain Res 1996;36:280–286. [CrossRef ]
6. Halbach O, Halbach V. BDNF effects on dendritic spine
morphology and
hippocampal function. Cell Tissue Res 2018;373:729–741.
[CrossRef ]
7. Panja D, Bramham CR. BDNF mechanisms in late LTP
formation: A synthesis
and breakdown. Neuropharmacology 2014;76:664–676.
[CrossRef ]
39. 8. Dougherty KD, Dreyfus CF, Black IB. Brain-derived
neurotrophic factor in
astrocytes, oligodendrocytes, and microglia/macrophages after
spinal cord
injury. Neurobiol Dis 2000;7:574–85. [CrossRef ]
9. Numakawa T, Suzuki S, Kumamaru E, Adachi N, Richards
M, Kunugi H.
BDNF function and intracellular signaling in neurons. Histol
Histopathol
2010;25:237–258. [CrossRef ]
10. Hwang J, Brothers RM, Castelli DM, Glowacki EM, Chen
YT, Salinas MM,
Kim J, Yung Y, Calvert HG. Acute high-intensity exercise-
induced cognitive
enhancement and brain- derived neurotrophic factor in young,
healthy
adults. Neurosci Lett 2016;630:247–253. [CrossRef ]
11. Hung CL, Tseng JW, Chao HH, Hung TM, Wang HS. Effect
of Acute Exercise
Mode on Serum Brain-Derived Neurotrophic Factor (BDNF) and
Task
Switching Performance. J Clin Med 2018;24;7:301. [CrossRef ]
12. Sartorius A, Hellweg R, Litzke J, Vogt M, Dormann C,
Vollmayr B, Danker-
Hopfe H, Gass P. Correlations and discrepancies between serum
and brain
tissue levels of neurotrophins after electroconvulsive treatment
in rats.
Pharmacopsychiatry 2009;42:270–276. [CrossRef ]
13. Yong KJ, Chang HH. The effect of exercise intensity on
brain derived
40. neurotrophic factor and memory in adolescents. Environ Health
Prev Med
2017;22:27. [CrossRef ]
14. Schmolesky MT, Webb DL, Hansen RA. The Effects of
Aerobic Exercise
Intensity and Duration on Levels of Brain-Derived Neurotrophic
Factor in
Healthy Men. J Sports Sci Med 2013;12:502–511.
15. Smith PJ, Blumenthal JA, Hoffman BM, Cooper H,
Strauman TA, Welsh-
Bohmer K, Browndyke JN, Sherwood A. Aerobic exercise and
neurocognitive
performance: a meta-analytic review of randomized controlled
trials.
Psychosom Med 2010;72:239–252. [CrossRef ]
16. Neeper SA, Gómez-Pinilla F, Choi J, Cotman CW. Physical
activity increases
mRNA for brain-derived neurotrophic factor and nerve growth
factor in rat
brain. Brain Res 1996;726:49–56. [CrossRef ]
17. Erickson KI, Prakash RS, Voss, L. Chaddock MW, Heo S,
McLaren M, Pence
BD, Martin SA, Vieira VJ, Woods JA, McAuley E, Kramer AF.
Brain-derived
neurotrophic factor is associated with age-related decline in
hippocampal
volume. J Neurosci 2010;30:5368–5375. [CrossRef ]
18. Knaepen K, Goekint M, Heyman EM, Meeusen R.
Neuroplasticity - exercise-
induced response of peripheral brain-derived neurotrophic
factor: a
41. systematic review of experimental studies in human subjects.
Sports Med
2010;40:765–801. [CrossRef ]
19. Griffin ÉW, Mullally S, Foley C, Warmington SA, O’Mara
SM, Kelly AM.
Aerobic exercise improves hippocampal function and increases
BDNF in the
serum of young adult males. Physiol Behav 2011;104:934–941.
[CrossRef ]
20. Skriver K, Roig M, Lundbye-Jensen J, Pingel J, Helge JW,
Kiens B, Nielsen JB.
Acute exercise improves motor memory: exploring potential
biomarkers.
Neurobiol Learn Mem 2014;116:46–58. [CrossRef ]
21. Tsai CL, Chen FC, Pan CY, Wang CH, Huang TH, Chen
TC. Impact of acute
aerobic exercise and cardiorespiratory fitness on visuospatial
attention
performance and serum BDNF levels.
Psychoneuroendocrinology
2014;41:121–131. [CrossRef ]
22. Slusher AL, Patterson VT, Schwartz CS, Acevedo EO.
Impact of high intensity
interval exercise on executive function and brain derived
neurotrophic factor
in healthy college aged males. Physiol Behav 2018;191:116–
122. [CrossRef ]
23. Chang YK, Labban JD, Gapin JI, Etnier JL. The effects of
acute exercise on
cognitive performance: a meta-analysis. Brain Res
2012;1453:87–101.
42. [CrossRef ]
24. Liu PZ, Nusslock R. Exercise-Mediated Neurogenesis in the
Hippocampus via
BDNF. Front Neurosci 2018;12:52. [CrossRef ]
25. Guiney H, Machado L. Benefits of regular aerobic exercise
for executive
functioning in healthy populations. Psychon Bull Rev
2013;20:73–86.
[CrossRef ]
26. Ruscheweyh R, Willemer C, Kruger K, Duning T,
Warnecke T, Sommer J, Ho
HV, Mooren F, Knecht S, Flöel A. Physical activity and
memory functions: an
interventional study. Neurobiol Aging 2011;32:1304–1319.
[CrossRef ]
27. Green MJ, Matheson SL, Shepherd A, Weickert CS, Carr
VJ. Brain-derived
neurotrophic factor levels in schizophrenia: a systematic review
with meta-
analysis. Mol Psychiatry 2011;16:960–72. [CrossRef ]
28. Castren E, Kojima M. Brain-derived neurotrophic factor in
mood disorders
and antidepressant treatments. Neurobiol Dis 2017;97:119–126.
[CrossRef ]
29. Park YM, Lee BH, Um TH, Kim S. Serum BDNF levels in
relation to illness
severity, suicide attempts, and central serotonin activity in
patients with
major depressive disorder: A pilot study. PLoS ONE
2014;9:e91061. [CrossRef ]
43. 30. Brunoni AR, Lopes M, Fregni F. A systematic review and
meta-analysis of
clinical studies on major depression and BDNF levels:
Implications for
the role of neuroplasticity in depression. Int J
Neuropsychopharmacol
2008;11:1169–1180. [CrossRef ]
31. Adlam J, Zaman R. The role of BDNF and memory in major
depressive
disorder. Psychiatr Danub 2013;25 Suppl 2:S368–S369.
32. Pandey GN, Dwivedi Y, Rizavi HS, Ren X, Zhang H,
Pavuluri MN. Brain-
derived neurotrophic factor gene and protein expression in
pediatric and
adult depressed subjects. Prog Neuropsychopharmacol Biol
Psychiatry
2010;34:645–651. [CrossRef ]
33. Brunoni AR, Lopes M, Fregni F. A systematic review and
meta-analysis of
clinical studies on major depression and BDNF levels:
Implications for
the role of neuroplasticity in depression. Int J
Neuropsychopharmacol
2008;11:1169–1180. [CrossRef ]
34. Cattaneo A, Bocchio-Chiavetto L, Zanardini R, Milanesi E,
Placentino
A, Gennarelli M. Reduced peripheral brain-derived neurotrophic
factor mRNA levels are normalized by antidepressant treatment.
Int J
Neuropsychopharmacol 2010;13:103–108. [CrossRef ]
44. 35. Kishi T, Yoshimura R, Ikuta T, Iwata N. Brain-Derived
Neurotrophic Factor and
Major Depressive Disorder: Evidence from Meta-Analyses.
Front Psychiatry
2018;8:308. [CrossRef ]
36. Orellana G, Slachevsky A. Executive Functioning in
Schizophrenia. Front
Psychiatry 2013;4:35. [CrossRef ]
37. Agartz I, Sedvall GC, Terenius L, Kulle B, Frigessi A, Hall
H, Jönsson EG. BDNF
gene variants and brain morphology in schizophrenia. Am J Med
Genet B
Neuropsychiatr Genet 2006;141:513–523. [CrossRef ]
38. Zhang XY, Liang J, Chen DC, Xiu MH, Yang FD, Kosten
TA, Kosten TR. Low
BDNF is associated with cognitive impairment in chronic
patients with
schizophrenia. Psychopharmacology 2012;222:277–284.
[CrossRef ]
39. Green MJ, Matheson SL, Shepherd A, Weickert CS, Carr
VJ. Brain-derived
neurotrophic factor levels in schizophrenia: a systematic review
with meta-
analysis. Mol Psychiatry 2011;16:960–972. [CrossRef ]
40. Zhang XY, Chen DC, Xiu MH, Haile CN, Luo X, Xu K,
Zhang HP, Zuo L, Zhang
Z, Zhang X, Kosten TA, Kosten TR. Cognitive and serum BDNF
correlates of
https://doi.org/10.1093/schbul/sbw115
https://doi.org/10.1073/pnas.1015950108
46. Gökçe et al. Exercise, BDNF and CognitionArch
Neuropsychiatry 2019;56:302−310
309
BDNF Val66Met gene polymorphism in patients with
schizophrenia and
normal controls. Hum Genet 2012;131:1187–1195. [CrossRef ]
41. Salomon JA, Vos T, Hogan DR, Gagnon M, Naghavi M,
Mokdad A, Begum N,
Shah R, Karyana M, Kosen S, Farje MR, Moncada G, Dutta A,
Sazawal S, Dyer
A, Seiler J, Aboyans V, Baker L, Baxter A, Benjamin EJ, Bhalla
K, Bin Abdulhak
A, Blyth F, Bourne R, Braithwaite T, Brooks P, Brugha TS,
Bryan-Hancock C,
Buchbinder R, Burney P, Calabria B, Chen H, Chugh SS,
Cooley R, Criqui MH,
Cross M, Dabhadkar KC, Dahodwala N, Davis A, Degenhardt L,
Díaz-Torné C,
Dorsey ER, Driscoll T, Edmond K, Elbaz A, Ezzati M, Feigin
V, Ferri CP, Flaxman
AD, Flood L, Fransen M, Fuse K, Gabbe BJ, Gillum RF,
Haagsma J, Harrison
JE, Havmoeller R, Hay RJ, Hel-Baqui A, Hoek HW, Hoffman H,
Hogeland E,
Hoy D, Jarvis D, Karthikeyan G, Knowlton LM, Lathlean T,
Leasher JL, Lim
SS, Lipshultz SE, Lopez AD, Lozano R, Lyons R, Malekzadeh
R, Marcenes W,
March L, Margolis DJ, McGill N, McGrath J, Mensah GA,
Meyer AC, Michaud
C, Moran A, Mori R, Murdoch ME, Naldi L, Newton CR,
Norman R, Omer
SB, Osborne R, Pearce N, Perez-Ruiz F, Perico N, Pesudovs K,
47. Phillips D,
Pourmalek F, Prince M, Rehm JT, Remuzzi G, Richardson K,
Room R, Saha
S, Sampson U, Sanchez-Riera L, Segui-Gomez M, Shahraz S,
Shibuya K,
Singh D, Sliwa K, Smith E, Soerjomataram I, Steiner T, Stolk
WA, Stovner LJ,
Sudfeld C, Taylor HR, Tleyjeh IM, van der Werf MJ, Watson
WL, Weatherall
DJ, Weintraub R, Weisskopf MG, Whiteford H, Wilkinson JD,
Woolf AD,
Zheng ZJ, Murray CJ, Jonas JB.. Common values in assessing
health outcomes
from disease and injury: disability weights measurement study
for the Global
Burden of Disease Study 2010. Lancet 2012;380:2129–2143.
[CrossRef ]
42. Keitner GI, Ryan CE, Solomon DA. Realistic expectations
and a disease
management model for depressed patients with persistent
symptoms. J Clin
Psychiatry 2006;67:1412–1421. [CrossRef ]
43. Hasan A, Falkai P, Wobrock T, Lieberman J, Glenthoj B,
Gattaz WF, Thibaut
F, Möller HJ; WFSBP Task Force on Treatment Guidelines for
Schizophrenia.
Guidelines for Biological Treatment of Schizophrenia, part 1:
update 2012
on the acute treatment of schizophrenia and the management of
treatment
resistance. World J Biol Psychiatry 2012;13:318–378. [CrossRef
]
44. Ramano E, Buys T, De Beer M. Formulating a return-to-
48. work decision
for employees with major depressive disorders: occupational
therapists’
experiences. Afr J Prim Health Care Fam Med 2016;8:954.
[CrossRef ]
45. Leutwyler H, Hubbard EM, Jeste DV, Miller B, Vinogradov
S. Associations of
schizophrenia symptoms and neurocognition with physical
activity in older
adults with schizophrenia. Biol Res Nurs 2013;16:23–30.
[CrossRef ]
46. Kimhy D, Vakhrusheva J, Bartels MN, Armstrong HF,
Ballon JS, Khan S,
Chang RW, Hansen MC, Ayanruoh L, Lister A, Castrén E,
Smith EE, Sloan
RP. The impact of aerobic exercise on brain-derived
neurotrophic factor and
neurocognition in individuals with schizophrenia: a single-
blind, randomized
clinical trial. Schizophr Bull 2015;41:859–68. [CrossRef ]
47. Nuechterlein KH, Ventura J, McEwen SC, Gretchen-Doorly
D, Vinogradov
S, Subotnik KL. Enhancing cognitive training through aerobic
exercise
after a first schizophrenia episode: theoretical conception and
pilot study.
Schizophr Bull 2016;42 Suppl 1:S44–S52. [CrossRef ]
48. Gourgouvelis J, Yielder P, Clarke ST, Behbahani H,
Murphy BA. Exercise Leads
to Better Clinical Outcomes in Those Receiving Medication
Plus Cognitive
Behavioral Therapy for Major Depressive Disorder. Front
49. Psychiatry
2018;9:37. [CrossRef ]
49. Vedovelli K, Giacobbo BL, Corrêa MS, Wieck A, Argimon
IIL, Bromberg E.
Multimodal physical activity increases brain-derived
neurotrophic factor
levels and improves cognition in institutionalized older women.
Geroscience
2017;39:407–417. [CrossRef ]
50. Kallies G, Rapp MA, Fydrich T, Fehm L, Tschorn M, Terán
C, Schwefel M,
Pietrek A, Henze R, Hellweg R, Ströhle A, Heinzel S, Heissel
A. Serum brain-
derived neurotrophic factor (BDNF) at rest and after acute
aerobic exercise
in majör depressive disorder. Psychoneuroendocrinology
2018;102:212–
215. [CrossRef ]
51. Salehi I, Hosseini SM, Haghighi M, Jahangard L, Bajoghli
H, Gerber M,
Puhse U, Holsboer-Trachsler E, Brand S. Electroconvulsive
therapy (ECT) and
aerobic exercise training (AET) increased plasma BDNF and
ameliorated
depressive symptoms in patients suffering from major
depressive disorder.
J Psychiatr Res 2016;76:1–8. [CrossRef ]
52. Schuch FB, Vasconcelos-Moreno MP, Borowsky C,
Zimmermann, AB,
Wollenhaupt-Aguiar B, Ferrari P, Almeida Fleck MP. The
effects of exercise on
oxidative stress (TBARS) and BDNF in severely depressed
50. inpatients. Eur Arch
Psychiatry Clin Neurosci 2014;264:605–613. [CrossRef ]
53. Meyer JD, Ellingson LD, Koltyn KF, Stegner AJ, Kim JS,
Cook DB.
Psychobiological Responses to Preferred and Prescribed
Intensity Exercise
in Major Depressive Disorder. Med Sci Sports Exerc
2016;48:2207–2215.
[CrossRef ]
54. Meyer JD, Koltyn KF, Stegner AJ, Kim JS, Cook DB.
Relationships between
serum BDNF and the antidepressant effect of acute exercise in
depressed
women. Psychoneuroendocrinology 2016;74:286–294.
[CrossRef ]
55. Borror A. Brain-derived neurotrophic factor mediates
cognitive
improvements following acute exercise. Med Hypotheses
2017;106:1–5.
[CrossRef ]
56. McMorris T, Hale BJ. Differential effects of differing
intensities of acute
exercise on speed and accuracy of cognition: a meta-analytical
investigation.
Brain Cogn 2012;80:338–351. [CrossRef ]
57. Loprinzi PD, Frith E. A brief primer on the mediational
role of BDNF in the
exercise-memory link. Clin Physiol Funct Imaging 2018;39:9–
14. [CrossRef ]
58. Gonzalez A, Moya-Alvarado G, Gonzalez-Billaut C,
51. Bronfman FC. Cellular
and molecular mechanisms regulating neuronal growth by brain-
derived
neurotrophic factor. Cytoskeleton (Hoboken) 2016;73:612–628.
[CrossRef ]
59. Zhao H, Alam A, San CY, Eguchi S, Chen Q, Lian Q, Ma
D. Molecular
mechanisms of brain-derived neurotrophic factor in neuro-
protection:
recent developments. Brain Res 2017;1665:1–21. [CrossRef ]
60. Vaynman S, Ying Z, Gomez-Pinilla F. Hippocampal BDNF
mediates the
efficacy of exercise on synaptic plasticity and cognition. Eur J
Neurosci
2004;20:2580–2590. [CrossRef ]
61. Kowiaski P, Lietzau G, Czuba E, Wakow M, Steliga A,
Mory J. BDNF. A Key
Factor with Multipotent Impact on Brain Signaling and Synaptic
Plasticity.
Cell Mol Neurobiol 2018;38:579–593. [CrossRef ]
62. Mahar I, Bambico FR, Mechawar N, Nobrega JN. Stress,
serotonin, and
hippocampal neurogenesis in relation to depression and
antidepressant
effects. Neurosci Biobehav Rev 2014;38:173–192. [CrossRef ]
63. López-Muñoz F, Alamo C. Monoaminergic
neurotransmission: the history
of the discovery of antidepressants from 1950s until today. Curr
Pharm Des
2009;15:1563–86. [CrossRef ]
52. 64. Duman R, Li N. A neurotrophic hypothesis of depression:
role of
synaptogenesis in the actions of NMDA receptor antagonists.
Philos Trans R
Soc Lond B Biol Sci 2012;367:2475–2484. [CrossRef ]
65. Björkholm C, Monteggia LM. BDNF - a key transducer of
antidepressant
effects. Neuropharmacology 2016;102:72–79. [CrossRef ]
66. Morichi S, Yamanaka G, Ishida Y, Oana S, Kashiwagi Y,
Kawashima H. Brain-
derived neurotrophic factor and interleukin-6 levels in the
serum and
cerebrospinal fluid of children with viral infection-induced
encephalopathy.
Neurochem Res 2014;39:2143–2149. [CrossRef ]
67. Wrann CD, White JP, Salogiannnis J, Laznik-Bogoslavski
D, Wu J, Ma D, Lin
JD, Greenberg ME, Spiegelman BM. Exercise induces
hippocampal BDNF
through a PGC-1alpha/FNDC5 pathway. Cell Metab
2013;18:649–659.
[CrossRef ]
68. Agudelo LZ, Femenía T, Orhan F, Porsmyr-Palmertz M,
Goiny M, Martinez-
Redondo V, Correia JC, Izadi M, Bhat M, Schuppe-Koistinen I,
Pettersson
AT, Ferreira DMS, Krook A, Barres R, Zierath JR, Erhardt S,
Lindskog M, Ruas
JL. Skeletal muscle PGC-1alpha1 modulates kynurenine
metabolism and
mediates resilience to stress-induced depression. Cell
2014;159:33–45.
53. [CrossRef ]
69. Krogh J, Rostrup E, Thomsen C, Elfving B, Videbech P,
Nordentoft M.
The effect of exercise on hippocampal volume and
neurotrophines in
patients with major depression - a randomized clinical trial. J
Affect Disord
2014;165:24–30. [CrossRef ]
70. Kerling A, Kück M, Tegtbur U, Grams L, Weber-
Spickschen S, Hanke A, Stubbs
B, Kahl KG. Exercise increases serum brain-derived
neurotrophic factor in
patients with major depressive disorder. J Affect Disord
2017;215:152–155.
[CrossRef ]
71. Toups MS, Greer TL, Kurian BT, Grannemann BD,
Carmody TJ, Huebinger
R, Rethorst C, Trivedi MH. Effects of serum Brain Derived
Neurotrophic
Factor on exercise augmentation treatment of depression. J
Psychiatr Res
2011;45:1301–1306. [CrossRef ]
72. Dinoff A, Herrmann N, Swardfager W, Gallagher D,
Lanctôt KL. The effect of
exercise on resting concentrations of peripheral brain-derived
neurotrophic
factor (BDNF) in major depressive disorder: A meta-analysis. J
Psychiatr Res
2018;105:123–131. [CrossRef ]
73. Dinoff A, Herrmann N, Swardfager W, Liu CS, Sherman C,
Chan S, Lanctôt
54. KL. The Effect of Exercise Training on Resting Concentrations
of Peripheral
Brain-Derived Neurotrophic Factor (BDNF): A Meta-Analysis.
PLoS ONE
2016;11:e0163037. [CrossRef ]
74. Do T, Kerr B, Kuzhikandathil EV. Brain-derived
neurotrophic factor regulates
the expression of D1 dopamine receptors. J Neurochem
2007;100:416–28.
[CrossRef ]
75. Castrén E, Kojima M. Brain-derived neurotrophic factor in
mood disorders
and antidepressant treatments. Neurobiol Dis 2017;97:119–126.
[CrossRef ]
https://doi.org/10.1007/s00439-012-1150-x
https://doi.org/10.1016/S0140-6736(12)61680-8
https://doi.org/10.4088/jcp.v67n0912
https://doi.org/10.3109/15622975.2012.696143
https://doi.org/10.4102/phcfm.v8i2.954
https://doi.org/10.1177/1099800413500845
https://doi.org/10.1093/schbul/sbv022
https://doi.org/10.1093/schbul/sbw007
https://doi.org/10.3389/fpsyt.2018.00037
https://doi.org/10.1007/s11357-017-9987-5
https://doi.org/10.1016/j.psyneuen.2018.12.015
https://doi.org/10.1016/j.jpsychires.2016.01.012
https://doi.org/10.1007/s00406-014-0489-5
https://doi.org/10.1249/mss.0000000000001022
https://doi.org/10.1016/j.psyneuen.2016.09.022
https://doi.org/10.1016/j.mehy.2017.06.024
https://doi.org/10.1016/j.bandc.2012.09.001
https://doi.org/10.1111/cpf.12522
https://doi.org/10.1002/cm.21312
56. neurotrophic factor with cognitive impairments and negative
symptoms in
schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry
2011;35:1836–
1840. [CrossRef ]
78. Khazaeinia T, Ramsey AA, Tam YK. The effects of
exercise on the
pharmacokinetics of drugs. J Pharm Pharm Sci 2000;3:292–302.
79. Campos C, Rocha NBF, Lattari E, Nardi AE, Machado S.
Exercise Induced
Neuroplasticity to Enhance Therapeutic Outcomes of Cognitive
Remediation
in Schizophrenia: Analyzing the Role of Brain Derived
Neurotrophic Factor.
CNS Neurol Disord Drug Targets 2017;16:638–651. [CrossRef ]
80. Woodward ML, Gicas KM, Warburton DE, White RF,
Rauscher A, Leonova O,
Su W, Smith GN, Thornton AE, Vertinsky AT, Phillips AA,
Goghari VM, Honer
WG, Lang DJ. Hippocampal volume and vasculature before and
after exercise
in treatment-resistant schizophrenia. Schizophrenia Res
2018;202:158–165.
[CrossRef ]
81. Thompson Ray M, Weickert CS, Wyatt E, Webster MJ.
Decreased BDNF, trkB-
TK+ and GAD67 mRNA expression in the hippocampus of
individuals with
schizophrenia and mood disorders. J Psychiatry Neurosci
2011;36:195–203.
[CrossRef ]
57. 82. Buchanan RW, Javitt DC, Marder SR, Schooler NR, Gold
JM, Mcmahon RP,
Heresco-Levy U, Carpenter WT. The Cognitive and Negative
Symptoms in
Schizophrenia Trial (Consist): the efficacy of glutamatergic
agents for negative
symptoms and cognitive impairments. Am J Psychiatry
2007;164:1593–602.
[CrossRef ]
83. Mattson MP. Glutamate and Neurotrophic Factors in
Neuronal Plasticity and
Disease. Ann N Y Acad Sci. 2008;1144: 97-112. doi:
10.1196/annals.1418.005
84. Wrann CD, White JP, Salogiannnis J, Laznik-Bogoslavski
D, Wu J, Ma D, Lin
JD, Greenberg ME, Spiegelman BM. Exercise induces
hippocampal BDNF
through a PGC-1alpha/FNDC5 pathway. Cell Metab
2013;18:649–659.
[CrossRef ]
85. Niitsu T, Shirayama Y, Matsuzawa D, Hasegawa T,
Kanahara N, Hashimoto T,
Shiraishi T, Shiina A, Fukami G, Fujisaki M, Watanabe H,
Nakazato M, Asano
M, Kimura S, Hashimoto K, Iyo M. Associations of serum
brain-derived
neurotrophic factor with cognitive impairments and negative
symptoms in
schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry
2011;35:1836–
1840. [CrossRef ]
86. Carlino D, Leone E, Di Cola F, Baj G, Marin R, Dinelli G,
58. Tongiorgi E, Vanna
MD. Low serum truncated-BDNF isoform correlates with higher
cognitive
impairment in schizophrenia. J Psychiatr Res 2011;45:273–279.
[CrossRef ]
87. Osby U, Westman J, Hallgren J, Gissler M. Mortality trends
in cardiovascular
causes in schizophrenia, bipolar and unipolar mood disorder in
Sweden
1987–2010. Eur J Public Health 2016;26:867–871. [CrossRef ]
88. Yang F, Wang K, Du X, Deng H, Wu HE, Yin G, Ning Y,
Huang X, Teixeira
AL, de Quevedo J, Soares JC, Li X, Lang X, Zhang XY. Sex
difference in the
association of body mass index and BDNF levels in Chinese
patients with
chronic schizophrenia. Psychopharmacology (Berl).
2019;236(2):753-762.
[CrossRef ]
89. Lommatzsch M, Zingler D, Schuhbaeck K, Schloetcke K,
Zingler C, Schuff-
Werner P, Virchow JC. The impact of age, weight and gender on
BDNF
levels in human platelets and plasma. Neurobiol Aging.
2005;26(1):115-23.
[CrossRef ]
90. Saucedo Marquez CM, Vanaudenaerde B, Troosters T,
Wenderoth N. High-
intensity interval training evokes larger serum BDNF levels
compared with
intense continuous exercise. J Appl Physiol (1985).
2015;15;119(12):1363-73.
60. in Media and Communication Studies
School of Health and Welfare, University of Halmstad,
Halmstad, Sweden
Abstract
Background: The mental health-care system in Sweden, as in
many other counties, has its main focus on the reduction of
psychiatric symptoms and the prevention of relapses. People
diagnosed with schizophrenia often have significant health
issues and experience reduced well-being in everyday life. The
social imaginary of mental illness as an imbalance of the brain
has implications concerning general attitudes in society. The
news media are an important source of information on
psychiatric disorders and have an important role in cultivating
public perceptions and stigma. News media can contribute
to the mental illness stigma and place individuals with mental
illnesses at risk of not receiving adequate care and support.
The aim of this preliminary study was to describe users’
experiences of housing support in everyday life.
Results: The results revealed three themes of housing support,
which were needed, but frequently insufficiently fulfilled
in the municipality. The three themes were: ‘‘Support to
Practice Healthy Routines in Daily Life,’’ ‘‘Support to Shape
Meaningful Contents in Everyday Life,’’ and ‘‘Support to Meet
Needs of Integrity and Respect.’’
Conclusions: The findings support previous studies arguing that
current health care and housing support fails to meet
basic needs and may lead to significant and unnecessary health
risks. Further investigation is needed regarding the links
between attitudes to mental illness in society and political and
financial principles for health care and housing support for
persons with schizophrenia. Further research is needed
regarding the role of the media in policymaking concerning
health
61. promotion interventions for people diagnosed with
schizophrenia.
Key words: Housing support, media, narratives, persons
diagnosed with schizophrenia, social sciences
(Accepted: 22 March 2016; Published: 9 May 2016)
The mental health-care system in Sweden, as in
many other counties, has a strong focus on the reduc-
tion of psychiatric symptoms and prevention of
relapses (Van Wel & Landsheer, 2011) in which posi-
tive dimensions of health have not been viewed as
suitable for evidence-based practice in health care
(Jormfeldt, 2011). Barriers regarding health promo-
tion among persons with severe mental illness have
been associated with stigma, as well as professional
and organizational obstacles in the health-care ser-
vices provided (Ehrlich et al., 2014). It has been
argued that the contemporary paradigm, which focuses
on neurological explanations regarding mental ill-
ness in society, fails to take psychological and rela-
62. tional explanations of mental illness into account
(Rose & Abi-Rached, 2013; Williams, Katz, &
Martin, 2011). The news media are an important
source of information on psychiatric disorders and
have an important role to play in cultivating public
perceptions and stigma (Klin & Lemish, 2008).
Previous research on news media content has estab-
lished that journalistic coverage of mental illness is
largely characterized by inaccuracies, exaggerations,
and misinformation and might even contribute to
mental illness stigma through negative news content.
For example, inaccurate stories on recovery may
promote the belief that mental illness cannot be
rehabilitated effectively (Wahl, 2003). News media
can contribute to the mental illness stigma by nega-
tive portrayals of individuals with these illnesses;
therefore, making them vulnerable to social rejection
and discrimination and at risk of not receiving
63. adequate care and support (Klin & Lemish, 2008).
People diagnosed with schizophrenia belong to a risk
Correspondence: H. Jormfeldt, School of Health and Welfare,
University of Halmstad, SE-301 18 Halmstad, Sweden. E-mail:
[email protected]
International Journal of
Qualitative Studies
on Health and Well-being
�
# 2016 H. Jormfeldt & M. Hallén. This is an Open Access
article distributed under the terms of the Creative Commons
Attribution 4.0 International
License (http://creativecommons.org/licenses/by/4.0/), allowing
third parties to copy and redistribute the material in any
medium or format and to remix,
transform, and build upon the material for any purpose, even
commercially, provided the original work is properly cited and
states its license.
1
Citation: Int J Qualitative Stud Health Well-being 2016, 11:
30571 - http://dx.doi.org/10.3402/qhw.v11.30571
(page number not for citation purpose)
http://creativecommons.org/licenses/by/4.0/
http://www.ijqhw.net/index.php/qhw/article/view/30571
http://dx.doi.org/10.3402/qhw.v11.30571
group for developing metabolic syndrome, cardio-
64. vascular disease, type 2 diabetes and reduced life
expectancy, as well as reduced well-being in every-
day life (Heald et al., 2010; Lassenius, Åkerlind,
Wiklund-Gustin, Arman, & Söderlund, 2013). The
causes of this risk are avoidable as it is related to
lifestyle in terms of inactivity, overweight, smoking,
and poor diet as well as the side effects of anti-
psychotic medication (Comptom, Daumit, & Druss,
2006). The general public, as well as policymakers,
frequently do not have sufficient knowledge of cur-
rent daily living conditions and the prerequisites for
health among people with severe mental illness.
People with mental disorders and their families are
acutely aware of the negative images of mental illness
in the news (and entertainment) media. However,
their perspectives about the prerequisites for health as
successful stories of recovery have rarely been in-
cluded as sources of news items (Stuart, 2006). The
65. aim of this preliminary study was to describe users’
experiences of housing support in everyday life.
Materials and methods
The sample in the present preliminary study con-
sisted of the members of the local service user
association, The Interest Alliance for Schizophrenia
and Allied Disorders. The local association embraces
approximately 50 members; involving people diag-
nosed with schizophrenia, their relatives, and others
with an interest regarding the particular diagnosis.
Forty-two letters with information about the purpose
of the study and an invitation to write down short
narratives concerning experiences of municipality sup-
port in everyday life were sent to all of the members
of the local service user association. The members
of the association were asked to recall situations
concerning municipality support in topics, such as
housekeeping, diet, physical activity, equality and
66. integrity, inclusion in society, participation in care
planning, health promotion and illness prevention,
and participation in meaningful activities or employ-
ment, as these topics where frequently highlighted
as problem areas during members? meetings in the
local association and thus appeared to be crucial to
health promotion from their perspective. Twenty-
four letters with narratives regarding experiences of
support in everyday life from the municipality came
in return during July and August, 2011. Five of the
letters with narratives were written by individuals
with personal experiences of housing support due to
mental disability, 14 letters were written by relatives
of persons receiving community support, and five
letters were written by members with experiences
of housing support among people diagnosed with
schizophrenia from a professional perspective.
The data were analyzed using a qualitative con-
67. tent analysis method, inspired by Graneheim and
Lundman (2004), and carried out by the first
author. The narratives were read several times to
become acquainted with the content. Meaning units
were identified, condensed, abstracted, and labeled
with a code. The codes were compared with each
other in order to identify similarities and differences
regarding the content of the narratives in relation to
the aim of the study. The findings were evaluated
by means of discussions among both authors with
regard to each step of the analysis.
Ethics
According to the Swedish Health Care Act (2003:
460), concerning the Ethical Review of Research
Involving Humans, an ethical review was not neces-
sary as participants were recruited among members
of the local organization and no sensitive personal
information was requested. Instead, only informa-
68. tion without links to a specific person regarding ex-
periences of the housing support provided by the
municipality was asked for. All of the participants
gave their informed consent verbally and by writing
down and sending their narratives to the authors.
Confidentiality was assured in accordance with World
Medical Association Declaration of Helsinki (2013).
Results
The narratives collected from the members of the
local service user association revealed three themes
regarding experiences of housing support in every-
day life support which were needed, but frequently
insufficiently fulfilled through municipality provi-
sion. The three themes were as follows: ‘‘Support
to Practice Healthy Routines in Daily Life,’’ ‘‘Sup-
port to Shape Meaningful Contents in Everyday
Life’’ and ‘‘Support to Meet Needs of Integrity and
Respect.’’
69. Support to Practice Healthy Routines in Daily Life
Relatives’ narratives indicated a lack of support on
the subject of routines concerning housekeeping,
diet, and physical activity. Narratives showed an
absence of support among service users in getting up
in the morning and not staying in bed all day as well
as a lack of support to maintain hygiene routines,
uphold physical activity, prepare regular meals, and
purchase nutritive food.
Several descriptions affirmed lack of support regard-
ing dietary interventions despite the evidence of the
lifesaving nature of these interventions. Narratives
H. Jormfeldt & M. Hallén
2
(page number not for citation purpose)
Citation: Int J Qualitative Stud Health Well-being 2016, 11:
30571 - http://dx.doi.org/10.3402/qhw.v11.30571
http://www.ijqhw.net/index.php/qhw/article/view/30571
http://dx.doi.org/10.3402/qhw.v11.30571
70. showed concerns because service users often eat
large portions and have an insufficient fiber intake in
combination with too much fat and sugar due to the
side effects of medical treatment.
Several descriptions revealed that obesity, which is
a well-known common issue related to antipsychotic
medication among people diagnosed with schizo-
phrenia, was seldom viewed as a serious matter
among municipality staff, even though these issues
require regular health checks by a physician. One
member of the user association*a relative of a
person diagnosed with schizophrenia*stated that:
The staff from the municipal social services
do not sufficiently recognize the needs of the
service users who, as a result, receive too little
encouragement to engage in activities and
recover.
Support to Shape Meaningful Contents in
Everyday Life
71. Narratives from both the relatives and from a pro-
fessional perspective revealed that service users seldom
received sufficient support in their daily tasks, which
was perceived as a drawback in their efforts to
become involved in the society. The housing support
provided by the municipality in the service users’
accommodations was described as ‘‘storage’’ instead
of care by the service users’ relatives. The realities
described by the narratives showed that the service
users often became too dependent upon their rela-
tives to be able to participate in society?s basic
activities, because support, company, and reassur-
ance from staff were absent. Another issue frequently
reported was the nonexistence of support or solu-
tions to service users’ difficulties to use public
transport. One relative expressed the following:
The service user does not have the same
opportunities to develop their capabilities . . .
they don’t get recognized and encouraged
72. enough to carry out things properly. They
simply don’t get help . . ..
Support to Meet Needs of Integrity and Respect
Some narratives spoke of the experiences of under-
standing and respectful behavior among staff, even
though an ‘‘us and them’’ perspective was evident in
most staff�user relationships, as well as experiences
of inequalities regarding power and decision-making.
Narratives of relatives expressed their experiences of
violations of both service users’ and their relatives’
dignity when staff were intruding their individual
integrity by claiming transparency regarding the ser-
vice user’s health status and personal relationships.
Narratives frequently described insufficient knowl-
edge among staff concerning the special difficulties
related to the diagnosis such as lack of motivation
and side effects of medical treatment. Moreover,
they easily accepted service users’ wishes to draw
73. back and isolate themselves without considering
the hostile effects of isolation, and the fact that the
diagnosis of schizophrenia often involves a tendency
to immure oneself. One service user described his
experiences as this:
The first years when I became ill I was just
assigned to an apartment and left all by myself
with prescribed medication. It took me several
years of misery before staff paid any attention
to my situation and gave me a hand to get
me back on track. Now I have got sufficient
support from staff but I should have got it from
the beginning.
Discussion
The lack of support regarding positive dimensions
of health among people with severe mental illness
has been revealed previously (Ehrlich et al., 2014;
Jormfeldt, 2011) and, according to the findings of
74. this preliminary study, this topic still needs attention.
The results of this preliminary study show that
current available housing support for people diag-
nosed with schizophrenia fails to meet basic needs
and may lead to significant and unnecessary health
risks and reduced well-being in line with previous
studies conducted by Comptom et al. (2006), Heald
et al. (2010), and Lassenius et al. (2013). There is a
reason to believe that stigma and barriers regarding
health promotion among people with severe mental
illness (Ehrlich et al., 2014) are related to the
negative media portrayals of mental illness (Wahl,
2003). Furthermore, the current focus on the reduc-
tion of psychiatric symptoms and prevention of
relapses in mental health care could be transformed
by media information concerning the fact that
mental illness can be rehabilitated effectively (Van
Wel & Landsheer, 2011). Further studies are needed
75. regarding the public discourse of mental illness in
public debate and within the scientific community to
increase awareness of how the current discourse
shapes the existing delivery of education, research,
and clinical praxis in mental health services. An
important topic in future research should be the role
of media portrayals of mental illness as it directly
affects people with mental illnesses by impeding
their social participation and interferes with their
recovery (Klin & Lemish, 2008). In addition, further
research is required regarding the perspective of
Experiences of housing support in everyday life
Citation: Int J Qualitative Stud Health Well-being 2016, 11:
30571 - http://dx.doi.org/10.3402/qhw.v11.30571 3
(page number not for citation purpose)
http://www.ijqhw.net/index.php/qhw/article/view/30571
http://dx.doi.org/10.3402/qhw.v11.30571
professionals in mental health services and journal-
ists focusing on mental health and illness.
76. Acknowledgments
We thank the members of the local user association
of The World Fellowship for Schizophrenia and
Allied Disorders, who generously shared their ex-
periences of housing support with us.
Conflict of interest and funding
The authors have not received any funding or
benefits from industry or elsewhere to conduct this
study.
References
Comptom, M., Daumit, G. L., & Druss, B. G. (2006). Cigarette
smoking and overweight/obesity among individuals with
serious mental illness. A preventive perspective. Harvard
Review of Psychiatry, 14, 212�222.
Ehrlich, C., Kendall, E., Frey, N., Kisely, S., Crowe, E.,
& Crompton, D. (2014). Improving the physical health
of people with severe mental illness: Boundaries of care
provision. International Journal of Mental Nursing, 23,
243�251.
77. Graneheim, U. H., & Lundman, B. (2004). Qualitative content
analysis in nursing research: Concepts, procedures and
measures to achieve trustworthiness. Nurse Education Today,
24, 105�112.
Heald, A., Montejo, A. L., Millar, H., De Hert, M., McCrae, J.,
& Correll, C. U. (2010). Management of physical health
in patients with schizophrenia: Practical recommendations.
European Psychiatry, 25, 41�45.
Jormfeldt, H. (2011). Supporting positive dimensions of health,
challenges in mental health care. International Journal of
Qualitative Studies on Health and Well-being, 6, 7126. doi:
http://dx.doi.org/10.3402/qhw.v6i2.7126
Klin, A., & Lemish, D. (2008). Mental disorders stigma in
the media: Review of studies on production, content, and
influences. Journal of Health Communication, 13(5), 434�
449. doi: http://dx.doi.org/10.1080/10810730802198813
Lassenius, O., Åkerlind, I., Wiklund-Gustin, L., Arman, M., &
Söderlund, A. (2013). Self-reported health and physical
activity among community mental healthcare users. Journal
78. of Psychiatric and Mental Health Nursing, 20, 82�90.
Rose, N., & Joelle, Abi-Rached, M. (2013). The New Brain
Sciences and the management of the mind. Princeton, NJ:
Princeton University Press.
Stuart, H. (2006). Media portrayal of mental illness and its
treatments: What effect does it have on people with mental
illness? CNS Drugs, 20, 99�106.
Swedish Health Care Act. (2003). The act concerning the ethical
review of research involving humans. Vetting the ethics of
research involving humans. Retrieved November 24, 2015,
from http://www.epn.se
Van Wel, T. F., & Landsheer, J. A. (2011). Societal
participation:
Examining the impact of a rehabilitation approach for young
people with schizophrenia. Journal of Psychiatric and Mental
Health Nursing, 19(9), 792�798.
Wahl, Otto, F. (2003). ‘News media portrayal of mental illness:
Implications for Public Policy.’ American Behavioral Scientist,
46(12), 1594�1600. doi: http://dx.doi.org/10.1177/0002764
203254615
Williams, S. J., Katz, S., & Martin, P. (2011). Neuroscience and
79. medicalisation: Sociological reflections on memory, medi-
cines and the brain. Sociological reflections on the neuros-
ciences. Advances in Medical Sociology, 13, 231�254.
World Medical Association Declaration of Helsinki. (2013).
Ethical principles for medical research involving human
subjects.
Retrieved November 24, 2015, from http://www.wma.net
H. Jormfeldt & M. Hallén
4
(page number not for citation purpose)
Citation: Int J Qualitative Stud Health Well-being 2016, 11:
30571 - http://dx.doi.org/10.3402/qhw.v11.30571
http://dx.doi.org/10.3402/qhw.v6i2.7126
http://dx.doi.org/10.1080/10810730802198813
http://www.epn.se
http://dx.doi.org/10.1177/0002764203254615
http://dx.doi.org/10.1177/0002764203254615
http://www.wma.net
http://www.ijqhw.net/index.php/qhw/article/view/30571
http://dx.doi.org/10.3402/qhw.v11.30571
Copyright of International Journal of Qualitative Studies on
Health & Well-Being is the
property of Co-Action Publishing and its content may not be
copied or emailed to multiple
sites or posted to a listserv without the copyright holder's
80. express written permission.
However, users may print, download, or email articles for
individual use.
PRAXIS Mini-Review Praxis 2014; 103(1): 2 7 - 3 2 27
Klinik für Forensische Psychiatrie, Psychiatrische
Universitätsklinik Zürich
Friederike Boudriot, Angela Guldimann, Elmar Habermeyer
Schizophrenie und Gewalt
Schizophrenia and Violence
Zusammenfassung
Schizophrene Menschen haben ein
gegenüber der Ällgemeinbevölkerung
erhöhtes Risiko, straffällig zu werden.
Der weitaus überwiegende Teil schi-
zophrener Patienten begeht jedoch
keine Straftaten und das Risiko, von
einer Gewalttat eines Schizophrenen
betroffen zu sein, ist für die Ällgemein-
bevölkerung gering. Die Ursachen von
Dehnquenz bei Schizophrenen sind
komplex, jedoch können bestimmte
Risikomerkmale (z.B. eine begleitende
Substanzabhängigkeit) benannt wer-
den. Die Behandelbarkeit und Legal-
prognose schizophrener Straftäter sind
gut, was dafür spricht, dass bei Risiko-
patienten durch Etablierung eines ge-
81. eigneten Helfernetzes auch präventiv
gearbeitet werden kann.
Schlüsselwörter: Schizophrenie - De-
linquenz - Gewalt - Risiko
Einleitung
Der Krankheitsbegriff der Schizophre-
nie geht auf den Schweizer Psychiater
Eugen Bleuler (1857-1939) zurück.
1911 veröffenthchte er seine richtungs-
weisende Monographie «Dementia
praecox oder Gruppe der Schizophre-
nien» mit der er diesen Begriff in der
medizinisch-psychiatrischen Fachwelt
verankerte [1]. Etymologisch setzt sich
der Begriff Schizophrenie aus den grie-
chischen Wörtern «schizo» (ich spalte)
und «phren» (Seele, Geist) zusammen.
Er beschreibt die «Spaltung» bzw. das
Äuseinanderfallen zentraler und übh-
cherweise integrierter geistig-seelischer
Funktionen wie Denken, Fühlen und
Wahrnehmung. Dementsprechend be-
schreiben auch die modernen diagnos-
tischen BGassifikationssysteme ICD-10
[2] und DSM-V [3] die Schizophrenie
als schwere psychische Erkrankung, die
durch Wahrnehmungsveränderungen
(z.B. Halluzinationen, Verkennungen,
Wahnwahrnehmungen) und Störungen
des Denkens (z.B. formale Denkstörun-
gen wie Gedankenabreissen, Gedan-
keneinschiebungen und Zerfahrenheit,
inhaltliche Denkstörungen mit Wahn-
82. bildungen, Ich-Störungen), des Fühlens
(z.B. verflachte oder unangemessene
Affekte) und des Handelns (z.B. Des-
organisation) imponieren. Hinsichtlich
der vorherrschenden Symptomatik, des
Verlaufes und der Prognose besteht eine
zum Teil erhebliche Heterogenität. Dies
findet Niederschlag in der Beschreibung
verschiedener Prägnanztypen, die je-
doch keine klar abgegrenzten Entitäten
darstellen und innerhalb des Langzeit-
verlaufes wechseln können [4].
Die Lebenszeitprävalenz schizophrener
Erkrankungen liegt kulturübergreifend
bei 0,6-1,0%. Beide Geschlechter sind
gleich häufig betroffen, Männer er-
kranken im Allgemeinen früher (15-25
Jahre) [5] als Frauen (25-35 Jahre). Die
Häufigkeit der Erkrankung und die auf-
grund des frühen Erkrankungsahers
langen Verläufe machen deutlich, dass
die Problematik nicht nur das psychia-
trische Fachgebiet betrifft, sondern für
viele medizinische Bereiche Relevanz
hat.
Die Ätiopathogenese der Schizophrenie
ist multifaktoriell [5]: Änlagebeding-
te genetische bzw. prä- und perinatal
erworbene Faktoren (Infektionen im
Mutterleib und/oder Geburtskomplika-
tionen) führen über neuronale Entwick-
lungsstörungen und damit verbundene
Veränderungen der Konnektivität zu
einer erhöhten Vulnerabilität. Lebens-
83. geschichtliche Belastungen und/oder
Substanzkonsum werden nachfolgend
als Auslöser der klinisch erkennbaren
Krankheitsentwicklung gesehen und
beeinflussen deren Verlauf Weitere
Ursachen der sehr unterschiedlichen
Krankheitsverläufe, die zwischen einer
weitgehenden Erholung (1/3 der Fälle)
und schweren Defizitsyndromen in ei-
nem weiteren Drittel schwanken kön-
nen, werden u.a. neurotoxische und
immunmodulatorische Prozesse disku-
tiert. Darüber hinaus ist wie bei vielen
potenziell chronischen Erkrankungen
die Compliance bezüglich der Medika-
menteneinnahme, aber auch der Grad
der Anpassung der individuellen Le-
bensbedingungen an die Gegebenheiten
der Erkrankung relevant.
Delinquenz
Das Krankheitsbild der Schizophrenie
ist mit vielen Vorurteilen belastet: In der
Ällgemeinbevölkerung aber auch bei
Psychologie- und Medizinstudenten zei-
Im Artikel verwendete Abkürzungen:
CI Konfidenzintervall
DSM-5 Diagnostisches und Statistisches
Manual Psychischer Störungen,
Fifth Edition
85. missbrauch noch einmal stärker erhöht
(OR für Schizophrene ohne Substanzab-
hängigkeit 2,1; 95%-CI 1,7-2,7; OR für
Schizophrene mit Substanzmissbraucb
8,9; 95%-CI 5,4-14,7).
Betrachtet man nicht nur die relativen
Risiken, sondern absolute Zahlen, dann
relativieren sich die vorgenannten Ergeb-
nisse: Trotz des erböhten Risikos, straf-
fällig zu werden, begeht nämlich nur ein
sehr kleiner Teü der Betroffenen, nämlich
ca. ein Patient pro 2000 Krankheitsfälle,
tatsächlich Gewaltdelikte. Das entspricht
bei einer für die Allgemeinbevölkerung
formulierten Basisrate von Gewaltstraf-
taten von 1:10000 zwar einem deutlich
erhöhten Risiko, die konkrete Gefähr-
dung für die Allgemeinbevölkerung
bleibt jedoch ausserordentlich gering: Bei
einer Prävalenz schizophrener Erkran-
kungen von 1% muss man 100 Personen
treffen, um einem Erkrankten zu begeg-
nen. Diese Zahl muss dann mit 2000
multipliziert werden, um die statistische
Wahrscheinlichkeit eines Kontaktes mit
einem gewaltbereiten Schizophrenen zu
erfassen. Das Risiko, einen gewaltberei-
ten schizophrenen Menschen zu treffen,
liegt somit bei 1:200000. Die Gefahr,
Opfer eines Gewaltdeliktes zu werden,
ist für die Allgemeinbevölkerung somit
niedrig [10].
Dennoch ist das Thema für den Leser-
kreis der PRAXIS nicht irrelevant, denn
die vorab dargestellten Berechnungen
86. haben wenig Relevanz für Angehörige
und für Mitarbeiter des medizinischen
Betreuungssystems. Da diese Personen
engere bzw. häufigere Kontakte zu Be-
troffenen haben, ist ihre Gefährdungsla-
ge eine andere: Studien konnten zeigen,
dass Opfer von Gewaltdelikten mehr-
heitlich Personen aus dem näheren Um-
feld waren, die Delikte wurden zumeist
in der eigenen Wohnung bzw. Wohnum-
gebung begangen (exemplarisch [11]).
Die Gefährdungen betreffen somit we-
niger die Allgemeinbevölkerung als viel-
mehr das persönliche Umfeld und pro-
fessionelle Helfer.
Mögliche Ursachen und
Erklärungsmodelle
Psychopathologie und Delinquenz
Das vorherrschende psychopathologische
Bild beeinfiusst die Ausgestaltung delin-
quenten Verhaltens bei Schizophrenen.
Entsprechend sind einige Prägnanztypen
schizophrener Erkrankungen und ver-
wandter Krankheitsbilder für die foren-
sische Psychiatrie besonders bedeutsam
(Tab. 1). In Anlehnung an diese Zusam-
menhänge wurden 1) impulsive Taten
mit starker Affektbeteiligung im Rabmen
akuter Positivsymptomatik, 2) geplante
(oft chronisch) wahnhaft motivierte Ta-
ten und 3) «dissozial» anmutende Taten
im Rahmen chronischer Verläufe mit so-
zialer Verwahrlosung, Kritikminderung
87. und Empathiemangel beschrieben [12].
Insbesondere für das Verständnis von
Gewalthandlungen im Rahmen akuter
Krankheitsstadien ist das Konzept der
sogenannten «threat/control-override»
Symptome relevant [13]. Hierbei han-
delt es sich um einen charakteristischen
Symptomenkomplex mit 1) bedrohlich
erlebten Icb-Störungen (Betroffene ha-
ben das Gefühl, in ihrem Denken und
Handeln von anderen kontrolliert, be-
einfiusst bzw. beherrscht zu werden) und
2) der wahnhaften und massiv ängsti-
genden Überzeugung, dass andere Men-
schen einem Schaden zufügen woüen. In
diesem Kontext spiegelt die Kriminah-
tät betroftener Personen Defizite in der
Realitätswahrnehmung bzw. -kontroUe
wider, die direkt auf sogenannte Positiv-
symptome zurückgehen.
Unabhängig davon können aber auch
sogenannte Negativsymptome in Form
von kognitiven Leistungseinbussen und
affektiven Veränderungen, die zu sozia-
lem Rückzug und defizitären Problem-
lösungsstrategien führen, Patienten in
Belastungssituationen, z. T. aber auch in
Alltagssituationen, massiv überfordern
und insbesondere zu Schwierigkeiten
bei der Einschätzung der Motive ihres
Gegenübers führen. Ausserdem kommt
es bei vielen chronischen Patienten im
Zuge der krankheitsbedingten Persön-
lichkeitsveränderung zu einem reduzier-
ten Empathievermögen, wie es schon Bl-
88. euler [1] als autistisches Grundsymptom
der Erkrankung beschrieben hat.
Es leuchtet unmittelbar ein, dass die
Auswirkungen der vorgenannten krank-
heitsbedingten Faktoren durch vorab
bestebende Persönlicbkeitsstörungen,
komorbiden Substanzkonsum, aber
auch durch krankheitsbedingten sozia-
len Abstieg mit nachfolgend akzentuier-
ten psychosozialen Schwierigkeiten und
einem fehlenden Hilfesystem verstärkt
werden können. Letztlich resultiert ein
Konglomerat unterschiedlicher Fakto-
ren, die im individuellen Zusammen-
spiel und mit unterschiedlicher Ausprä-
gung zur Delinquenz eines Betroftenen
beitragen.
Neurobiologische Aspekte
Es gibt inzwischen zahlreiche Befunde
zu genetischen, neurophysiologischen
und morphologischen Veränderungen,
die mit schizophrenen Erkrankungen
einerseits und/oder mit aggressivem Ver-
halten andererseits in Verbindung stehen
PRAXIS Mini-Review Praxis 2014; 103(1): 27-32 29
Tab. 1: Forensisch-relevante Subtypen
ïUDtypen
Paranoide
Schizophrenie
91. (Übersicht bei Kalus [14]). Spezifische
Auslöser bzw. hirnorganische Läsionen,
die Gewalt begünstigen können, sind da-
bei jedoch (noch) nicht identifiziert wor-
den. Vielmehr ergibt sich eine den vorab
dargestellten komplexen ätiologischen
Bedingungen ähnliche Konstellation,
bei der es vorwiegend um neurobiolo-
gische Vulnerabilitäten geht, die je nach
Lebenssituation und Krankheitsverlauf
in unterschiedlicher Art und Intensität
verhaltenswirksam werden können. Da-
bei sind jene Hirnstrukturen, die gene-
rell mit Aggressivität im Zusammenhang
stehen, zu einem beträchtlichen Teil
identisch mit jenen, die bei scbizopbre-
nen Erkrankungen alteriert sind (orbi-
tofrontaler Cortex, anteriorer cingulärer
Cortex, Basalganglien und Amygdala).
Gleicbes gilt für die Neurotransmitter
Dopamin und Serotonin, wobei bei schi-
zophrenen Erkrankungen bzgl. Dopa-
min in limbischen Hirnarealen, die für
Flucht und Gegenwehr zuständig sind,
eine Uberaktivität und in den frontalen
Regionen, die für die Verhaltenshem-
mung bzw. -kontroUe relevant sind, ein
Serotoninmangel vorliegt.
Die biopsychosozialen Wechselwirkun-
gen zwischen Lebensereignissen, Ver-
baltensstilen bzw. neurobiologischen
Faktoren und die daraus resultierenden
Entstehungsmechanismen aggressiven
Verhaltens bei schizophrenen Menschen
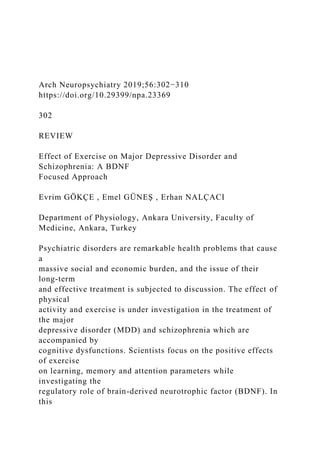
![review, the effect of aerobic exercise on peripheral BDNF
levels in MDD
and schizophrenia is examined by including human studies in
which
acute and chronic aerobic exercise are applied. The results
showed that
aerobic exercise caused different responses on BDNF levels,
and some
of the studies were accompanied by the improvement in
cognitive
functions in BDNF changes. In order to comprehend the effect
of aerobic
exercise in MDD and schizophrenia, it is understood that
applying
studies on larger and paired participant groups with different
exercise
frequencies and tensions in necessary.
Keywords: Brain derived neurotrophic factor, aerobic exercise,
schizophrenia, major depressive disorder, cognitive functions
ABSTRACT
Cite this article as: Gökçe E, Güneş E, Nalçacı E. Effect of
Exercise on Major Depressive Disorder and Schizophrenia: A
BDNF Focused Approach. Arch Neuropsychiatry
2019;56:302-310.
302
Correspondence Address: Emel GÜNEŞ, Ankara Üniversitesi
Tıp Fakültesi, Fizyoloji Anabilim Dalı, Ankara, Turkey • E-
mail: [email protected]
Received: 04.09.2018, Accepted: 27.03.2019, Available Online
Date: 15.10.2019](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)