
Recommended
More Related Content
What's hot
What's hot (19)
Similar to Dose modification fasting
Similar to Dose modification fasting (20)
More from Ibn Abdullah
More from Ibn Abdullah (20)
Recently uploaded
Recently uploaded (20)
Dose modification fasting
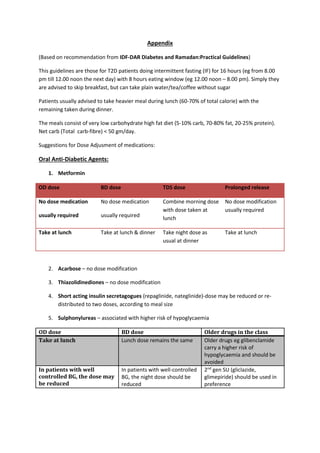
- 1. Appendix (Based on recommendation from IDF-DAR Diabetes and Ramadan:Practical Guidelines) This guidelines are those for T2D patients doing intermittent fasting (IF) for 16 hours (eg from 8.00 pm till 12.00 noon the next day) with 8 hours eating window (eg 12.00 noon – 8.00 pm). Simply they are advised to skip breakfast, but can take plain water/tea/coffee without sugar Patients usually advised to take heavier meal during lunch (60-70% of total calorie) with the remaining taken during dinner. The meals consist of very low carbohydrate high fat diet (5-10% carb, 70-80% fat, 20-25% protein). Net carb (Total carb-fibre) < 50 gm/day. Suggestions for Dose Adjusment of medications: Oral Anti-Diabetic Agents: 1. Metformin OD dose BD dose TDS dose Prolonged release No dose medication usually required No dose medication usually required Combine morning dose with dose taken at lunch No dose modification usually required Take at lunch Take at lunch & dinner Take night dose as usual at dinner Take at lunch 2. Acarbose – no dose modification 3. Thiazolidinediones – no dose modification 4. Short acting insulin secretagogues (repaglinide, nateglinide)-dose may be reduced or re- distributed to two doses, according to meal size 5. Sulphonylureas – associated with higher risk of hypoglycaemia OD dose BD dose Older drugs in the class Take at lunch Lunch dose remains the same Older drugs eg glibenclamide carry a higher risk of hypoglycaemia and should be avoided In patients with well controlled BG, the dose may be reduced In patients with well-controlled BG, the night dose should be reduced 2nd gen SU (gliclazide, glimepiride) should be used in preference
- 2. 6. SGLT-2 inhibitors – no dose adjustment 7. DPP-4 inhibitors – no dose adjustment Insulin Treatment for T2DM This may include the use of a long acting/intermediate acting basal insulin (insulin glargine, insulin determir or NPH insulin), possibly with a rapid or short-acting bolus/pre-meal insulin (lispro, aspart or regular human insulin) Changes to long and short acting insulin dose during IF Long/intermediate-acting (basal insulin) Short acting insulin NPH/detemir/glargine/degludec once daily Reduce dose by 15-30% Take at lunch Omit morning dose Normal dose at lunch Reduce dinner dose by 25-50% NPH/determir/glargine twice-daily Take usual morning dose at lunch Reduce evening dose 50% and take at dinner Dose modification based on dextrostix: Fasting/pre-lunch/pre-dinner dxt Pre-lunch Pre-lunch/pre-dinner Basal insulin Short acting insulin < 3.9 mmol/L or symptoms Reduce by 4 units Reduce by 4 units 3.9-5.0 mmol/L Reduce by 2 units Reduce by 2 units 5.0-7.2 mmol/L No change required No change required 7.2-11.1 mmol/L Increase by 2 units Increase by 2 units >11.1 mmol/L Increase by 4 units Increase by 4 units
- 3. Changes to pre-mixed insulin dosing during intermittent fasting Once daily dosing Twice daily dosing Three times daily dosing Take normal dose at lunch Take normal dose at lunch Omit morning dose. Adjust lunch and dinner dose Reduce dinner dose by 25-50% Carry out dose titration every 3 days (see below) Fasting/pre-lunch/pre-dinner dxt Pre-mixed insulin modification <3.9 mmol/L or symptoms Reduce by 4 units 3.9-5.0 mmol/L Reduce by 2 units 5.0-7.0 mmol/L No change required 7.0-11.1 mmol/L Increase by 2 units >11.1 mmol/L Increase by 4 units