Japnese Enchephalitis Virus
•Download as PPTX, PDF•
3 likes•164 views

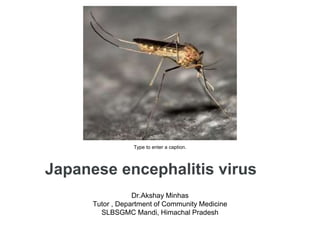
Japnese Enchephalitis Virus is spread by Culex Mosquitoe.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Japnese Enchephalitis Virus
Similar to Japnese Enchephalitis Virus (20)
Recently uploaded
Recently uploaded (20)
Japnese Enchephalitis Virus
- 1. Japanese encephalitis virus Dr.Akshay Minhas Tutor , Department of Community Medicine SLBSGMC Mandi, Himachal Pradesh Type to enter a caption.
- 2. Type to enter a caption.
- 3. Key facts Japanese encephalitis virus (JEV) is a flavivirus related to dengue, yellow fever and West Nile viruses, and is spread by mosquitoes. JEV is the main cause of viral encephalitis in many countries of Asia with an estimated 68 000 clinical cases every year. Although symptomatic Japanese encephalitis (JE) is rare, the case- fatality rate among those with encephalitis can be as high as 30%. Permanent neurologic or psychiatric sequelae can occur in 30%– 50% of those with encephalitis. 24 countries in the WHO South-East Asia and Western Pacific regions have endemic JEV transmission, exposing more than 3 billion people to risks of infection. There is no cure for the disease. Treatment is focused on relieving severe clinical signs and supporting the patient to overcome the infection. Safe and effective vaccines are available to prevent JE.
- 4. Introduction Japanese encephalitis virus JEV is the most cause of viral encephalitis in Asia. It is a mosquito-borne flavivirus, and belongs to the same genus as dengue, yellow fever and West Nile viruses. The first case of Japanese encephalitis viral disease (JE) was documented in 1871 in Japan. The annual incidence of clinical disease varies both across and within endemic countries, ranging from <1 to >10 per 100 000 population or higher during outbreaks. A literature review estimates nearly 68 000 clinical cases of JE globally each year, with approximately 13 600 to 20 400 deaths. JE primarily affects children. Most adults in endemic countries have natural immunity after childhood infection, but individuals of any age may be affected.
- 5. Ecology and Epidemiology Type to enter a caption.
- 6. Ecology and epidemiology 24 countries in the WHO South-East Asia and Western Pacific regions have JEV transmission risk, which includes more than 3 billion people. JEV is transmitted to humans through bites from infected mosquitoes of the Culex species (mainly Culex tritaeniorhynchus). The virus is transmitted in an enzootic cycle among mosquitoes and amplifying vertebrate hosts, chiefly ardeid (wading) birds and domestic pigs . Humans are incidental hosts as transmission from human-to-mosquito is not possible because of low levels of viraemia found in humans, making humans dead-end hosts.
- 7. Culex mosquitoes, primarily C. tritaeniorhynchus, are the principal vectors. Both male and female mosquitoes feed on plant fluids and nectar. However, the female typically requires a blood meal from a warm-blooded animal before a viable batch of eggs can be laid, and only the female is capable of sucking blood and it bite mainly in night.
- 8. Type to enter a caption.
- 9. The geographic spread of JE may be related to increasing international trade and travel, and global warming could permit overwintering in more temperate regions. JEV is transmitted seasonally in most areas of Asia, but there are, in broad terms, two epidemiological patterns. In northern (temperate) regions, JEV is transmitted during the summer months, around May to September. In southern (subtropical and tropical) regions, the virus is largely endemic, with sporadic outbreaks throughout the year, peaking at the start of the rainy season. Across affected Asia-Pacific countries, approximately 67 900 clinical cases of JE are documented per year; of these, an estimated 13 600 to 20 400 deaths occur annually .
- 10. Five different genotypes have been identified with genotype 3 having historically been the most common; however, genotype 1 is becoming a more common circulating genotype. The major JEV genotypes have varying overlap in geographical distribution but all belong to the same serotype and are similar in terms of virulence and host preference . Incidence of disease can fluctuate as JE transmission varies from year to year. Historically thought to be a childhood disease, the annual incidence of JE in those younger than 15 years of age is an
- 11. The highest mortality rate from JE is in Uttar Pradesh where children’s deaths in Gorakhpur recently sent shock waves all over the country. These deaths were primarily attributed to JE aggravated by poor healthcare facilities. Since 2010, India has seen 10,893 JE cases and 1,756 deaths, a mortality rate of 17 per cent. Due to a large variation across regions, incidence in those younger than 15 years of age may be as high as an estimated 12.6/100 000 in some high incidence areas in China and the Democratic People’s Republic of Korea.
- 12. In some countries even without vaccination programmes, such as Bangladesh, a substantial proportion of cases are in those older than 15 years of age . In Thailand, 69% of individuals 20–24 years had protective levels of neutralising antibody, and by 40 years of age, approximately 90% of the population had protective levels of antibody titers. Among a sample of unvaccinated 12–18 year- olds in the Philippines, the seroprevalence rate was just 44%.
- 13. These data suggest an important proportion of adults are still susceptible. How severity differs by age group is not well understood, in part because of the lack of follow up of many cases. The age-specific incidence may be considered when designing immunisation programmes, and some countries, such as Nepal and India , have chosen to conduct campaigns in which all individuals over one year
- 14. Who is at risk? • Residents of rural areas in endemic locations • Those who are deployed to work on those areas • Usually its not spread in Urban areas but due
- 15. Signs and symptoms Incubation period: – Normally 5 to 15 days JEV infections are mild (fever and headache) or without apparent symptoms, but approximately 1 in 250 infections results in severe clinical illness.
- 16. Most infections are asymptomatic; however, clinical cases can rapidly progress to severe symptoms with an estimated 30% of survivors experience long-term neurologic abnormalities and serious disabilities. Of all clinical cases, 20–30% die, and the risk of severe disease and death in children younger than 10 years is even higher.
- 17. Diagnosis Individuals who live in or have travelled to a JE-endemic area and experience encephalitis are considered a suspected JE case. To confirm JEV infection and to rule out other causes of encephalitis requires a laboratory testing of serum or, preferentially, cerebrospinal fluid. Surveillance of the disease is mostly syndromic for acute encephalitis. Confirmatory laboratory testing is often conducted in dedicated sentinel sites, and efforts are undertaken to expand laboratory- based surveillance. Case-based surveillance is established in countries that effectively control JE through vaccination.
- 18. Treatment & Prevention and control There is no antiviral treatment for patients with JE. Treatment is supportive to relieve symptoms and stabilize the patient. Safe and effective JE vaccines are available to prevent disease. WHO recommends having strong JE prevention and control activities, including JE immunization in all regions where the disease is a recognized public health priority, along with strengthening surveillance and reporting mechanisms. Even if the number of JE- confirmed cases is low, vaccination should be considered where there is a suitable environment for JE virus transmission. There is little evidence to support a reduction in JE disease burden from interventions other than the vaccination of humans.
- 19. There are 4 main types of JE vaccines currently in use: inactivated mouse brain- derived vaccines, inactivated Vero cell- derived vaccines, live attenuated vaccines, and live recombinant vaccines. Over the past years, the live attenuated SA14-14-2 vaccine manufactured in China has become the most widely used vaccine in endemic countries, and it was prequalified by WHO in October 2013. Cell-culture based inactivated vaccines and the live recombinant vaccine based on the yellow fever vaccine strain have also been licensed and WHO-prequalified.
- 20. In November 2013, GAVI opened a funding window to support JE vaccination campaigns in eligible countries. All travellers to Japanese encephalitis- endemic areas should take precautions to avoid mosquito bites to reduce the risk for JE. Personal preventive measures include the use of repellents, long-sleeved clothes, coils and vaporizers. Travellers spending extensive time in JE endemic areas are recommended to get vaccinated.
- 21. JE Vaccine in India JE Vaccination :113 JE endemic districts have completed the JE mass vaccination and are implementing JE under routine vaccination. 2nd dose of JE is also introduced in RI in JE endemic states since April, 2013 National Vector borne Disease control Program Division (NVBDCP) has identified 62 new JE endemic Districts. JE campaign in these new districts targeting children between 1-15 years of age is planned in a phased manner. Uttar Pradesh, West Bengal, Karnataka, Assam and Bihar.
- 22. What you can do? Environmental Control Environment manipulation : elimination of breeding spaces, filling and drainage operation, carefully planned water management, provision of piped water supply, proper disposal of refuse and other waste, intensive cleaning in and around houses. Personal Protection against mosquito bite : Mosquito net, screening , repellents . Chemical Control Wide range of insecticides are available but due to resistance and environmental pollution they are not effective . Newer generations insecticides like methoxychlor, abate and dursban are recommended as they are biodegradable . Biological Control To minimise environmental pollution with toxic chemical biological control like fish(Gambusia), bacteria, fungi , protozoa and viruses are under study. Although these may pose a direct hazard to the health of man himself.
- 23. Control of piggeries Integrated Approach Culex. quinquefasciatus, best controlled by improving sanitation and installing modern sewage systems, but often this is not feasible and integrated approach to be implemented .
- 24. Disease outbreaks Major outbreaks of JE occur every 2-15 years. JE transmission intensifies during the rainy season, during which vector populations increase. However, there has not yet been evidence of increased JEV transmission following major floods or tsunamis. The spread of JEV in new areas has been correlated with agricultural development and intensive rice cultivation supported by irrigation programmes. “Herd immunity” cannot be attained through vaccination due to the zoonotic nature of the virus — it remains in the environment.
- 25. Thank You Please subscribe health and family channel On youtube which will keep us motivated to provide more heath related information to you and your family Eggs of culex mosquito in water