
Recommended
More Related Content
What's hot
What's hot (20)
Similar to AMOEBIC LIVER ABSCESS
Similar to AMOEBIC LIVER ABSCESS (20)
More from DR.P.S SUDHAKAR
More from DR.P.S SUDHAKAR (20)
Recently uploaded
Recently uploaded (20)
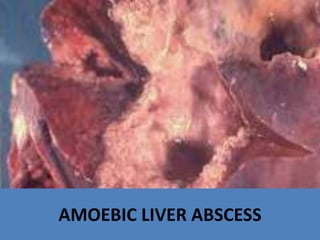
AMOEBIC LIVER ABSCESS
- 2. • Amebic liver abscess is caused by Entamoeba histolytica. • This parasite causes amebiasis, an intestinal infection that is also called amebic dysentery. • After an infection has occurred, the parasite may be carried by the bloodstream from the intestines to the liver.
- 3. • It is also called Tropical abscess ( dysenteric abscess). • It is the commonest extra-intestinal manifestation of amoebiasis.
- 4. Aetiopathogenesis • This disease is caused by Entamoeba histolytica. • It is almost always a complication of amoebic dysentery. • This can occur in the acute stage or in the chronic carrier stage Infection from the caecum (typhlitis) spreads through the tributary of superior mesenteric vein. From sigmoid colon, through the tributary of inferior mesenteric vein.
- 6. • The right branch of the portal vein is in direct line with the portal vein. • Hence, by streamline phenomenon organisms reach the right lobe more often than the left lobe. • The right lobe is also much bigger than the left lobe.
- 7. • In the right lobe, it is the posterosuperior surface which gets involved because it is extraperitoneal (bare area of liver). • It has no peritoneal covering.
- 8. • After reaching the liver, the organism causes destruction of hepatocytes by releasing powerful cytolytic enzymes resulting in liquefaction necrosis. • It also causes aseptic thrombosis of blood vessels resulting in necrosis of liver tissue.
- 9. • At the same time, some RBCs are also broken down. • This causes anchovy sauce pus, which is chocolate brown in colour, and is a mixture of broken down RBCs, hepatocytes, etc.
- 10. • Green pus is referred to pus mixed with bile, which is seen in a few patients. • In majority of the cases, pus is sterile. Secondary infection occurs in about 20 to 30% of the cases.
- 11. • Amoebae are rarely present in the pus but are present in the wall of the abscess cavity. • The wall contains monocytes, plasma cells, lymphocytes and fibroblasts. • Abscesses are multiple which fuse to form a single large abscess cavity in about 70% of the cases.
- 12. • Due to perihepatitis, abscess gets fixed to the diaphragm resulting in immobility of the diaphragm. • Liver abscess in the left lobe gets adhered to anterior abdominal wall.
- 13. Amoebic infection of gall bladder and bile does not occur because of deleterious effect of bile on amoebae.
- 14. Clinical features • Male alcoholics are commonly affected, in the age group of 20-40 years. • It is eight times more common in men. • Seen in patients with low socioeconomic status. • Severe pain in the right hypochondrium is due to the enlarged liver. This stage is called stage of Amoebic Hepatitis. • If USG is done, it may not demonstrate any abscesses but there may be many microabscesses. • At this stage, there is low grade fever, weakness, anorexia, etc.
- 15. Clinical features • High grade fever with chills and rigors develop if the stage proceeds to pyogenic liver abscess due to secondary bacterial infection of amoebic abscess. • Thoracic symptoms such as nonproductive cough, pleurisy and right shoulder pain are common.
- 16. Signs • Anaemia, emaciation, toxic look and an earthy complexion is present. • Jaundice may be present if abscesses are multiple, due tocompression of biliary radicles. • However, it is rare ( 15% ). • It is of cholestatic variety. • Liver is enlarged in the right hypochondrium, tender and soft (liver enlarges in upward direction)
- 17. Signs • Intercostal tenderness differentiates it from acute cholecystitis. • Intercostal oedema can also be present
- 18. Investigations 1. Total WBC count may be increased if there is secondary infection. 2. Stool examination for ova and cysts of Entamoeba histolytica may be positive in 25% of cases. 3. Serologic testing: The indirect haemagglutination test is positive in 90-95% of patients with an amoebic abscess.
- 19. Investigations 4. Screening chest: When the patient is asked to take a deep breath, right side of the diaphragm does not move due to inflammatory (perihepatitis) adhesions between liver and diaphragm. This is called homolateral immobility of the diaphragm. A small pleural effusion may also be present.
- 20. Investigations 5. Sigmoidoscopy may demonstrate large, deep amoebic ulcers-flask shaped. 6. Abdominal USG: It is the investigation of choice. • To locate site of abscess and then to confirm diagnosis. • Ultrasound guided needle aspiration can also be done and biopsy of abscess wall should be taken. • Multiple abscesses can be made out.
- 21. Investigations 7. CT scan can demonstrate an abscess cavity as a low density zone surrounded by peripheral hypodense zone due to inflammatory reaction.
- 22. Treatment • lt can be classified into: I. Conservative II. Ultrasound-guided aspiration and pigtail drainage III. Surgery-drainage
- 23. I. Conservative line of management • It is indicated in amoebic hepatitis. Tab. Metronidazole 400-800 mg, 3 times a day is given for 14 days. • The only recognisable side-effect is metallic taste. • If the condition does not improve, injection Emeline 1 mg/kg body weight to a total of 60 mg/day deep IM for a maximum of 6 days is given.
- 24. II. US-guided needle aspiration/pigtail catheter drainage • It is indicated in cases of amoebic liver abscess. • Before it is aspirated, bleeding profile (BT, CT, PT) should be normal and injection vitamin K 10 mg, IM should be given for at least 3 days. • US-guided aspiration is also the treatment of choice where metronidazole is contraindicated, e.g. 1st trimester of pregnancy.
- 25. II. US-guided needle aspiration/pigtail catheter drainage • It can be easily done under local anaesthesia • Can be repeated, if pus recollects. • Typically it is anchovy sauce pus. Aspiration is followed by insertion of pig tai I catheter. • Before removal of the catheter do a repeat ultrasound to check for residual pus.
- 26. Pigtail catheter drainage of amoebic liver abscess-it is a nonoperative method of treatment Ultrasound is done to check residual abscess cavity
- 27. Ill. Surgery (open drainage) and laparoscopic Indications 1. Failure of US-guided needle aspiration. 2. Ruptured amoebic liver abscess with amoebic peritonitis.
- 28. Complications of amoebic liver abscess • Amoebic peritonitis, resulting in acute abdomen with shock. • It has to be treated like any peritonitis-laparotomy, drainage of pus and drain the abscess cavity to outside (possibility of amoebiasis cutis is still present but rare). • Rupture into pleural space causing pleural effusion. • Rupture into the bronchus resulting in coughing out anchovy sauce (may be a natural cure )-bronchopleural fistula. • Amoebic pericardia! effusion occurs due to rupture of left liver lobe abscess into pericardia! space.
- 30. • Belladonna: This remedy is most often indicated for the initiatory symptoms of abscess. The parts swell rapidly, become bright red, there is intense throbbing which is painful,pus develops speedily the swelling increases and the redness radiates.
- 31. • Hepar Sulphur : It is great homeopathic remedy for suppurations where the pus is not decomposed. It suits especially lymphatic, phlegmatic individuals. Excessive sensitiveness of the parts is a leading indication.
- 32. • Silicea: This remedy is indicated where the suppuration continues and the wound refuses to heal, no matter where the suppurative process is located; the pus is apt to be thin, watery and the process is sluggish and indolent one. Under Silicea the suppurative process takes on a healthy action, the pus becomes benign, granulation appear.
- 33. • Mercurius: Differing from Belladonna, from Hepar, and especially from Silicea is Mercurius, which is one of our good remedies in abscess. It comes in after Belladonna, when pus has formed. It favors the formation of pus especially in the lower potencies, and is especially indicated in glandular abscesses; the pus is greenish in tint, and quite thin and fluid.