2020 parm 2223 u5 introduction to central venous access
•Download as PPTX, PDF•
3 likes•262 views

Ain introduction to pre existing central venous access for paramedic students, as well as the basics of infusion devices.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to 2020 parm 2223 u5 introduction to central venous access
Similar to 2020 parm 2223 u5 introduction to central venous access (20)
More from Robert Cole
More from Robert Cole (20)
Recently uploaded
Recently uploaded (20)
2020 parm 2223 u5 introduction to central venous access
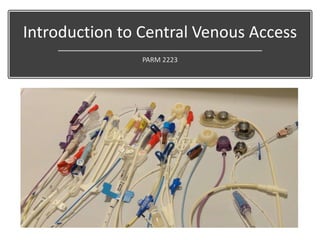
- 1. Introduction to Central Venous Access PARM 2223
- 2. Objectives • Compare and contrast types of vascular access devices Non-central lines (but treated like central lines): – Midline Central Lines – PICC – Tunneled Central Line – Non-Tunneled Central venous Line – Port-a-cath • Discuss indications and procedures for accessing a vascular access device in the prehospital setting.
- 3. What is a Vascular Access Device? • Central venous access devices are small, flexible tubes placed in large central veins for people who require frequent access, large volumes, or special medications to the bloodstream. • They allow medications to be delivered directly into larger veins, are less likely to clot, and can be left in for long periods.
- 4. Central Venous Access • Catheters are often named by: – Location – Name of the particular catheter – Name of the inventor of the catheter or insertion technique • Although tip location of all central lines may be (virtually) the same, insertion sites and methods may vary.
- 5. Why not a peripheral line? • Longer term therapy (beyond 14 days) • Repeated Venipunctures • Increased risk of phlebitis, infection, or occlusion • Medication Preclusions (relative) – Other compounds (TPN) • PH <5 or >9 or Hyper- osmolar
- 6. Why a central line? • For long term therapy (7 days to lifetime) • Benefits: – Located in the central vasculature – Better medication distribution? – Any drug that can be given IV can go in central line • Other considerations – Surgical procedure for some – It is a potential entry portal for infection into central circulation
- 7. PASV-Pressure Activated Safety Valve • PASV-Pressure Activated Safety Valve (PASV can be on a PICC, tunneled or non- tunneled line) – Three-way valve in external hub of catheter – Saline or heparin – Pulsatile (start/stop) technique when flushing – Once weekly flushing when not in use – No clamps
- 8. Midline • For short term therapy – peripheral – For short term generally 4 weeks – Limits – same as Peripheral catheters • It is places in the same place as a PICC line but it ends prior to the axilla so it is a peripheral IV • Benefits – Good for all ages – Good for intermittent infusions – Lasts a little longer than traditional peripheral IV so less restart
- 9. Peripheral Inserted Central Catheter
- 10. Peripheral Inserted Central Catheter • A IV catheter, typically placed in a large peripheral vein, but the catheter is much longer. • It ends in the central circulation. • In many settings the PICC line has become the preferred alternative to central lines due to cost effectiveness, ease of insertion and significanly lower incidence of major complications • Neonates to the elderly All Central Catheters can be Single, double, or triple lumen
- 11. Valved vs. Unvalved PICCs • Valved PICCS – Have no clamps. – Have a valve that prevents blood reflux into the catheter. – Do not require heparin for flushing. – Are saline-only lines • NAMES: Groshong, PASV and Power PICC Solo
- 12. TUNNELED CENTRAL VENOUS CATHETERS
- 13. Tunneled Central Venous Catheter • Tunneled Central Venous Catheters: • Single, double or triple lumen device, surgically tunneled through subcutaneous tissue to an exit site generally on the chest or abdominal wall. – The tip rests in the vena cava. – A cuff that lies in the subcutaneous tunnel, around which fibrous tissue grows, helps to secure the device. • Tunneling reduces infection risk. • Can be hidden under clothing which is good for body image
- 14. Word of Caution: • When removing clothing, be cognizant not to displace or cut these lines.
- 16. Non- Tunneled Central Venous Catheter • Central venous access for infusion of vasoactive drugs, TPN, high dose KCl, etc. – Hemorrhagic disorder where large volumes blood/blood products needed – Hemodynamic Monitoring – Need for frequent blood draws where peripheral access limited. • Lack of peripheral venous access • Ease of bedside emergent insertion • Non-Tunneled small-bore catheters are for short term use 5-10 days, rotate at 21 days. Generally sutured for duration.
- 17. Common sites Femoral Catheter IJ Catheter – Internal Jugular Subclavian Catheter
- 18. Implanted Ports
- 19. Implanted Ports Advantages: • Cosmetic • Lowest risk of infection • Allow activity • Easy for at home care by caregivers and patients
- 21. Implanted Ports • Limitations – Requires a minor surgical procedure for placement and removal. – Medication delivery requires injection through skin – Can get a port pocket, tunnel, or sepsis infection • Ideally requires special needles
- 22. Implanted Ports – Huber needles
- 24. Did you know paramedics used to start central lines?
- 25. Basic Principles of EMS access • No , seriously. Pay attention to sterility of procedure, not of gloves. • Clean ports TWICE - 15 seconds each time. • Hand Hygiene!! Sterile Procedures Only in crisis • Heparin • At lease 5 cc, until you see blood Aspirate before flushing
- 26. Use a 10 cc syringe • Always use a 10ml or larger syringe to flush or administer medications. • Smaller syringes have increased flushing pressure that can cause catheter rupture.
- 27. Migration • Most catheters are marked and their “depth” known. – Conceptually, similar to an ETT tube. – A catheter that migrates externally should never be readvanced into the vein. – Re-advancing it could dislodge it, punctiure a major vessel, or introduce infection. • It should be stabilized at the point of external migration and assessed for proper placement before further use. – If catheter appears to have migrated a CXR may be indicated for confirmation of placement.
- 29. Seriously…Maintain sterility as much as possible
- 30. Arterial Lines
- 32. Lines used for Hemodynamic Monitoring
- 33. Invasive Hemodynamic Monitoring • Squarely in the critical care realm • Pressure monitoring may or may not be hooked up for transport. – May be confused for normal central line • Becoming less common • Do not access or use for medication administration without specific orders and training
- 35. Art line for hemodynamic monitoring
- 36. Bottom Line: Don’t mess with invasive hemodynamic monitoring lines without specialized training
- 37. INFUSION DEVICES
- 38. What we will talk about • Gravity Infusion Devices • Volumetric Infusion Pumps • Syringe Pumps • Patient Controlled Analgesia Pumps • Elastomeric Pumps
- 39. Gravity Infusion Devices • Most common method of IVF administration in prehospital arena and overseas. – Flow by gravity – Controlled by a “clamp” – With and without filter • Pros: – Simple – Inexpensive • Cons – Accuracy +/- 15% – No safety procedures – No smart features
- 40. Have you considered: • Viscosity of fluid affects flow rate • Changes in height will change flow rate. • Position of piggyback fluids can change flow rate • Position of iste can change flow rate
- 41. Buretrol • AKA: Volutrol, Burette • Most are 150 cc • Most are 60 cc • Precise volumes • Safety flow to prevent air • Still a gravity flow
- 43. IV Infusion Pumps Volumetric Pump Syringe Pump
- 44. Singe vs. Multi channel pumps
- 45. Syringe Pumps • Two Types – Research/Industrial Syringe Pumps • Ultra small volumes – Medical Syringe Pumps • FDA reviewed and approved • With and without “smart pump” technology
- 47. Drip Assist
- 48. PCAs
- 49. What are “Smart Pumps”? • No “single point failure” – No single cause can cause the pump to fail to operate correctly without an alarm or simply stoping – Minimum requirement for smart pumps
- 50. Other Features • Battery Backup • Anti-free flow • Up stream and down stream occlusion • Air in Alarm • “Drug Library” with limits and alarms • Other features • Log of events • Anti-tamper features
- 51. Elastomeric Pump • “Medicine Balls”, “Ball Pumps” , “Grenade Pumps” and “Balloon Pumps” • Portable and disposable • No electronics • Not dependent on gravity – Must still be kept within a certain range • Can be subject to temperature fluctuations • Pre-set rate through a “flow restrictor” • Often “filled” in a hospital pharmacy for home care.
- 52. Used for • Home care • Administration of: – Chemo – Antibiotics – Non Opioid Pain medications – Post surgical care
- 57. Questions?
Editor's Notes
- A central line is a type of catheter that is placed in a large vein that allows multiple IV fluids to be given and blood to be drawn. When compared to a typical IV line, a central line is larger, can stay in place longer, can deliver a greater volume of fluids and allows blood to be drawn easily. A central line can also be used to measure fluid volume status, and to help determine if a patient is dehydrated or has received an adequate amount of fluid to support bodily functions.
- PASV-Pressure Activated Safety Valve (PASV can be on a PICC, tunneled or non-tunneled line) Three-way valve in external hub of catheter Saline or heparin Pulsatile (start/stop) technique when flushing Once weekly flushing when not in use No clamps
- A midline is not a central line.
- A PICC line, a type of IV access that can be maintained for weeks and months, is not a central line but shares many characteristics with this type of IV access.
- PICC is an acronym for a Peripherally Inserted Central Catheter, and it is, in essence, a long IV line. It is usually inserted in a smaller vein in the upper arm (peripheral), and terminates in a larger vein in the chest near the heart (central). “Catheter” is just another name for “tube” in the medical lexicon. By definition, and per its’ acronym, A PICC line is a peripherally inserted central catheter. It is a long (approx. 50cm or 20 inches) slender flexible tube that is inserted into a peripheral vein, typically in the upper arm of adults and children and sometimes the scalp and lower extremity of pediatric patients. The PICC is then threaded along the vein into the subclavian and eventually into the vena cava and central circulation. The Paramedic should understand that a PICC is a central venous access device (CVAD) which requires the same care as other central venous catheters to avoid complications and achieve positive patient outcomes Major complications such as hemothorax, pneumothorax, and vessel rupture are not typically present with PICC insertion. In addition risk of infection is greatly reduced due to the mere placement of the line: upper arm, verses neck or chest for central line.
- PICC lines are generally classified into either open ended or valved. An open ended catheter is generally maintained with a Heparin lock solution because of blood reflux into the catheter tip. With a valved catheter, a valve is built into the internal tip or external hub. o The valve prevents blood from the vessel from inadvertently entering the catheter. While these valves have different designs and function in different ways, the one common aspect is the fact that they can be flushed and locked with 0.9% Normal Saline solution only and do not require heparin. Examples of these types of valved catheters are the o Groshong Catheter o Bard Solo PICC o Vaxcel PASV PICC line placement can be done in both the inpatient and outpatient setting and is performed by trained and qualified health care professionals such as : o Radiologists o Physician assistants and certified o Certified Registered Nurses. The Basilic vein is preferred because of its large diameter; however the Cephalic vein can be used. Least preferred are the Brachial veins due to increased risk of complications.
- Tunneled Central lines •Long-term catheters •OK for blood draws & any kind of IV Therapy •Tunneled under the skin to decrease infection and accidental removal. •In home care have had patients cut with scissors •Pt/CG learns site care, cap change and flushing. A tunneled central venous catheter is a long silicone or polyurethane tube open at each end. It is inserted into a central vein at one location (neck, chest or groin) and tunneled under the skin to a separate exit site, typically the chest. It exits the body several inches away from the vein. A Dacron cuff, located and anchored just under the skin at the exit site, provides stability and helps reduce risks of infection. Though more comfortable and discreet for patients than non-tunneled catheters, they still carry the same risks of hemorrhage, pneumothorax, and infection. Infection rates are reported to be lower with tunneled catheters verses non-tunneled catheters. With proper care a tunneled catheter can remain in place for several years. Tunneled catheters are often referred to by their brand name, o Hickman o Hohn o Broviac o Leonard o Neostar o Groshong They are available in single, double and triple lumens depending on brand. Tunneled catheters are generally surgically placed or placed in radiology. In some facilities, highly trained infusion nurses are also performing the procedure. o As such, they are not able to be removed in the home.
- Non-tunneled catheters are placed by physicians, radiologists and other trained health care professionals in an acute care setting. They are inserted by direct venipuncture into the internal jugular, subclavian, and femoral veins. The risk of pneumothorax and other complications are such that catheter placement needs to be in a setting where emergency intervention is readily available. The risk of infection is significantly higher than that of other CVADs due to the fact that bacterial count in the area of insertion is much higher than other body areas. They are typically inserted for short tem use and are not recommended for home use due to the higher incidences of complications.
- Femoral: Dirty location •Increase Infection •Easy to pull/fall out •Least comfortable for patients and staff
- Advantages of implanted ports: •They are cosmetically appealing and preserve body image •Lowest risk of infection of all chest-accessed central lines •Allow patients to carry on virtually all activities including bathing and swimming when it is not in use •Ports do not require exit-site care, when not accessed •Weekly needle change and daily flush when in use •Monthly access and flush not in use •Generally used in adults •Seen primarily in Oncology patients Limits: •Requires a minor surgical procedure for placement and removal. •Medication delivery requires injection through skin •Can get a port pocket, tunnel, or sepsis infection
- Implantable ports are implanted subcutaneously to provide access to the peritoneal cavity or the vascular, arterial, or epidural system. The use of implantable ports has grown tremendously since their first use in 1981. Oncology patients were the first recipients of implanted ports. Acceptance of these devices has grown rapidly with more than 100,000 ports being implanted each year. More than fourteen different manufacturers have designed their own type of port, yet most are similar in design, function, and application.
- The implantable port consists of the portal body and the catheter. o The portal body is made of stainless steel, titanium, polysulfone, or a combination thereof with an inner center space called a reservoir. o Most catheters are made of silicone, as this material is known to produce fewer thrombi. The three principal outside features of the I.P. are the base, the shoulder, and the barb. A self-sealing, compressed silicone septum, overlays the portal body. The septum is designed for either top and/or side access. Port access is done by an I.P. needle, Huber needle, or a needle with a deflective, non-coring tip. Several commercially made ports are available in single or double lumen designs. Dual ports allow infusion of non-compatible medications and fluids. o Additional IV access increases the probability of complications such as phlebitis, hematomas, and infiltration. Lower profile (thinner) designs are available for smaller patients.
- The IP should be accessed with the smallest gauge noncoring safety needle, or Huber needle, necessary to accommodate the prescribed therapy. To reduce the risk of needle dislodgement while accessed, the Huber needle should: o be a length that allows the needle to make contact with the back of the port when inserted and sit flush to the skin and secure within the port. INS recommends replacement of non-coring needle every 7 days when left in place for continuous infusions. The type of I.P. needle used differs with each facility. Huber needles come in various length and gauge and with and without catheters attached.
- 1.May be used if unable to establish a peripheral IV or IO in patients with a systolic BP < 80 mmHg. 2. May be used if the patient is in cardiac arrest and not able to establish a peripheral IV or IO. 3. Do NOT administer benzodiazepines (i.e. Valium or Versed) via central line. 4. A 10 mL syringe or larger must be used when accessing any central line to prevent excess infusion pressure that could damage the internal wall of the catheter. 5. Always aspirate 5 ml of blood from the central line and discard prior to administration of medications or IV fluids to remove Heparin from the line. 6. Strictly adhere to aseptic technique when handling a central line: Cleanse injection port twice with an alcohol prep (using a new alcohol prep each time) prior to accessing. 7. Do not remove the injection cap. 8. Do not allow IV fluids to run dry. 9. Always expel all air from syringes and IV tubing prior to administration. 10. Should damage occur to the external catheter, immediately clamp the catheter between the skin and damaged area.
- https://youtu.be/43cbxXOH33k Video on “FLUSHING A MIDLINE or CVAD v2”
- An arterial line (also art-line or a-line) is a thin catheter inserted into an artery. It is most commonly used in intensive care medicine and anesthesia to monitor blood pressure directly and in real-time (rather than by intermittent and indirect measurement) and to obtain samples for arterial blood gas analysis.
- Gravity infusion devices depend on gravity to drive the infusion. The system consists of an administration set containing a drip chamber and utilizing a roller clamp to control flow which is measured by counting the dropsGravity infusions are ideal for infusing fluids which do not need to be infused with absolute precision
- The story of Christopher (1632-1723), microscopist, physiologist, artist and renown architect, Wren, using a quill and a pig’s bladder, created the first working IV infusion device. His first experiment, in 1658, was to instil a mixture of wine, ale, opium and liver of antimony into a dog’s veins. The dog tolerated it remarkably well and the experiment was repeated with other infusates. However, a series of problems emerged which forced an evolution in Wren’s technology. As Felts notes, the ‘study of the circulation of experimental animals was difficult in the beginning because vascular access was limited by blood clotting and primitive equipment. Quills could not be easily fixed into blood vessels and were neither firm nor durable enough. Silver, however, was malleable and firm, so that pipes of varying calibres could be fashioned and their ends rimmed for anchoringwith ligatures. Such improved instrumentation allowed the exploration of many hitherto unplumbed fields by injection studies and administration of many agents’ (13). It was Richard Lower, Wren’s colleague, who devised the new instruments and took over the transfusion work from the architect when he left Oxford to design his churches
- Ideal for austere enviroments Used in Africa during Ebola outbreak Works with IV fluid and blood 1% accurace
- Certified to have no single point of failure. That is, no single cause of failure should cause the pump to silently fail to operate correctly. It should at least stop pumping and make at least an audible error indication. This is a minimum requirement on all human-rated infusion pumps of whatever age. It is not required for veterinary infusion pumps. Batteries, so the pump can operate if the power fails or is unplugged. Anti-free-flow devices prevent blood from draining from the patient, or infusate from freely entering the patient, when the infusion pump is being set up. A "down pressure" sensor will detect when the patient's vein is blocked, or the line to the patient is kinked. This may be configurable for high (subcutaneous and epidural) or low (venous) applications. An "air-in-line" detector. A typical detector will use an ultrasonic transmitter and receiver to detect when air is being pumped. Some pumps actually measure the volume, and may even have configurable volumes, from 0.1 to 2 ml of air. None of these amounts can cause harm, but sometimes the air can interfere with the infusion of a low-dose medicine. An "up pressure" sensor can detect when the bag or syringe is empty, or even if the bag or syringe is being squeezed. A drug library with customizable programmable limits for individual drugs that helps to avoid medication errors. Mechanisms to avoid uncontrolled flow of drugs in large volume pumps and increasingly also in syringe pumps (piston-brake) Many pumps include an internal electronic log of the last several thousand therapy events. These are usually tagged with the time and date from the pump's clock. Usually, erasing the log is a feature protected by a security code, specifically to detect staff abuse of the pump or patient. Many makes of infusion pump can be configured to display only a small subset of features while they are operating, in order to prevent tampering by patients, untrained staff and visitors.
- Also known as “homeballs,” “ball pumps,”or “grenade pumps.” An elastomeric pump is a device that infuses medication once the tubing is unclamped. Built with an elastic balloon inside a very tough outer cover, the device pushes intravenous medication through tubing and a filter that is attached to the reservoir. The pharmacy fills the devices with your medication in a sterile environment then ships them to you, ready to use. It infuses at a specified rate. There are several advantages to infusing your medication in this way. The storage and stability of the drug is longer since these can be refrigerated or frozen, depending on the medication. The elastomeric pump does not run by gravity as a regular IV does. It is totally portable so you are not attached to an IV pole; it can be carried in a pocket or pouch. Because the device comes with tubing, you will not need to use additional IV tubing for the infusion, decreasing your expense and manipulation of the system, which decreases chances of introducing an infection. The liquid eventually goes through the flow restrictor and then out into the connection with the patient. The pressure will be consistent in level until the infusion is nearly over, which is when there is usually a pressure spike that results in a slightly higher rate of flow. The flow restrictor controls the accuracy of the rate of flow. The flow restrictor is typically a steel cannula or glass capillary which is molded into the system tubing or even placed inside the elastomeric reservoir. Elastomeric pumps do not need electricity, nor are they driven by gravity. When a pump is placed below or above a patient, the rate of flow will often decrease or increase thanks to the head height effect.
- The balloon is where the chemotherapy is held. The balloon has two layers: an inner membrane that holds the chemotherapy and an outer cover that protects the inner membrane. The fill port is where the chemotherapy is put into the balloon. The fill port has a cap that protects it. The infusion line carries chemotherapy from the balloon to your CVC tubing. The clamp is used to start and stop the flow of chemotherapy. The filter filters the chemotherapy before it’s infused into your body. The flow restrictor helps to control how quickly the chemotherapy is infused. The patient connector is where the infusion line connects to your CVC tubing. The patient connector has a cap that covers the connector when it’s not connected to your CVC tubing. It’s removed when the pump is connected to your CVC tubing.