
Recommended
Recommended
More Related Content
More from bobbywlane695641
More from bobbywlane695641 (20)
Recently uploaded
Recently uploaded (20)
cost and end-of-life care • summer 2011 121The Ethical .docx
- 1. cost and end-of-life care • summer 2011 121 The Ethical Implications of Health Spending: Death and Other Expensive Conditions Dan Crippen and Amber E. Barnato Overview In this essay I ask the reader to consider the “end of life” as a life stage, rather than as a health state. At one end of the life course is childhood and at the other end is elderhood. The basic inter-generational social compact in most societies is that working adults take care of their children and their parents, and count on their children to do the same for them. In developed countries, these obligations are met in part through government programs, with taxpayers funding signifi- cant portions of education, health care, and income support. The financing of these public programs, in addition to other public services, involves ethically charged trade-offs. In the United States, public outlays on behalf of children and the elderly span roughly the same number of years, but with very different levels of spending. Cross-sectionally, transfers from work- ers (via taxes) go more to the elderly in the form of Medicare and Social Security income than to children
- 2. in the form of public education and means-tested health insurance (e.g., Medicaid, SCHIP). Longitu- dinally, delayed “transfers” to these same children are manifest as better or worse economic conditions once the children become workers. If current workers, in addition to providing for the young and old through taxpayer-funded social programs, manage to save as well by reducing their own consumption of goods and services, then future generations are likely to be better off since these current savings are invested in capital which will allow the economy to grow (faster). In con- trast, if individuals, institutions, or governments bor- row for consumption today, then future generations are likely to be worse off since current consumption may reduce economic growth in the future and, in the case of public borrowing, additionally obligate future taxpayers to fund the cost of expenditures we make today. In the United States, health care spending is a criti- cal component of examining both these intra- and inter-generational transfers. At present we spend much more on health care, and in total, for the elderly, Dan Crippen, Ph.D., is the newly appointed Executive Di- rector of the National Governors Association. He has held various posts in the public sector, including Chief Counsel to the Senate Majority Leader, Assistant to the President and Domestic Policy Advisor, and Director of the Congressional Budget Office. Over the last decade, he has worked primarily in the private sector with various organizations providing or financing health care. Amber E. Barnato, M.D., M.P.H., M.S., is an Associate Professor of Medicine and Health Policy and Management at the University of Pittsburgh, and was a Visiting Scholar at the Congressional Budget Office during Dan Crippen’s tenure as Director.
- 3. 122 journal of law, medicine & ethics S Y M P O S I U M than we do for educating and ensuring safety-net health care for our youth, thus posing the question of whether we are spending “enough” on the young. Moreover, by incurring large budget deficits at the fed- eral level, in part to continue supporting health care for the elderly (which constitutes a large and growing part of the total budget), we are pushing off the pay- ment for some of current health care spending on the elderly to future generations. The primary driver of increased health care costs for the elderly is not spending for those who died, but spending for all beneficiaries. Secular trends in Medicare spending reveal that spending on behalf of beneficiaries who die during the year has been a stable 27% for decades. Although those who die incur a dis- proportionate share of total spending, the drivers of cost growth affect survivors and decedents identically. Increasing health care spending on the elderly who are in the “end of life” life-stage (not just the “end of life” health state) will crowd out investments in current and future generations of children. The inter-generational impact of health care spending on those who are in the “end of life” life stage may have greater ethical impli- cations than the narrow “futility” debate surounding those who are in the “end of life” health state. The Issue Giving, and accepting, the assistance of others is a com-
- 4. mon human experience. Whether as children, when education and the essentials of life are provided by adults, or as retirees who receive financial and physi- cal aid in their later years, virtually all of us experience both the give and take of life. Historically, much of this support has been voluntarily provided by familial sup- port and bequests, or by charitable contributions and institutions, including those of the church. In more successful societies with higher income, the elderly may also have savings to consume in retirement. One of the hallmarks of “economically developed” civilizations is a large component of public, govern- mental transfer of resources, from those who are working to those who are largely not. In most coun- tries both culture and government shape these trans- fers, subject to societal and legal compacts between and across generations. Altogether, these public and private reallocations of resources can consist of real property (land, housing, public roads), financial resources (credit and cash), or transfers, including direct services (bequests, educa- tion, health care). In the United States, children are provided a combi- nation of public and private resources. The lion’s share of funding for education, especially through high school, comes from state and local taxes. The provi- sion of food, clothing, housing, and health care are mostly provided by parents, but federal programs for food stamps, school lunch programs, housing vouch- ers, Medicaid, and SCHIP contribute to lower-income families.
- 5. The elderly are typically supported with public pro- grams of cash transfers, primarily social security, and reimbursement for health care through Medicare and Medicaid. By increasing amounts, governments of all types are providing income and health care for their former employees, now retirees. Altogether, public programs for health care provide nearly half of the annual costs for all health care in the United States. The funding for these programs, including for retir- ees, comes largely from taxes on current workers, or from borrowing. The moral or ethical implications of these realloca- tions, might be examined across both current popu- lations (living citizens of differing ages, for example), as well as across generations over longer periods of time. As there are always a finite number of resources at a given point in time, current spending reflects the choices we make among those in the current popula- tion who cannot fend for themselves — for example, the more we spend on our parents after they retire, the less we have for our children. The basic compact in the United States between the current working population and their dependents has been that workers pay or provide for their children and help support their parents. As workers retire, they depend on their working children to pay taxes to sup- port them through public programs, whatever private transfers they receive, and a ready market to sell the non-cash assets they have accumulated. As support moves from private and familial to public and govern- mental, the association between workers and depen- dents becomes less direct since the reallocations occur within the larger society.
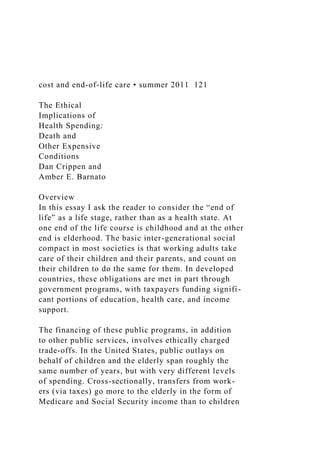
- 6. Figure 1 illustrates the typical pattern in the United States of consumption of resources, either directly or as provided by others, and the creation of resources as reflected by labor income. The total available for consumption is determined by the total production of goods and services of those working, i.e., the size of the economy. Across the current population the amount consumed is approximately a zero-sum game: the more consumption for any one group — children, workers, retirees — means less for the others. The basic compact can be altered in many ways, the most important of which affects future generations. In basic terms, if the current working population not only pays for their children and supports their parents, but cost and end-of-life care • summer 2011 123 Crippen and Barnato also saves a portion of their income, then economic growth can be accelerated and future economies will be larger, thus making it easier to assist future depen- dent populations. Savings add to the capital available, making it easier (and cheaper) to provide investment that increases national output. It is important to note that it is national savings that counts — the total of individuals, business, government, non-profits — and borrowing by any sector reduces the positive effect of savings by others. Similarly, if borrowing is used to fund today’s consump- tion of goods and services,
- 7. future spending and saving will be reduced. In the case of gov- ernment borrowing, especially by the federal government, it is possible to push the costs of debt well into the future. For example, current inter- est costs on the federal debt are nearly $200 billion. With the expected deficits over the next decade, interest is pro- jected to grow to $800 billion — nearly as much as the total for Medicare in 2020. That means federal spending will need to be cut, taxes increased, or additional debt incurred to cover just the interest on our debt. As we continue to increase debt, future generations will have less to spend and invest. To the extent the spend- ing and borrowing of government is needed/used to fund health care, the country is pushing the cost of today’s health care onto future citizens. Under cur- rent policies, the present cohort of children will be expected to pay not only for their own children and parents, but also for past generations as well, breaking the basic intergenerational compact. Figure 1 Life-Cycle Income and Consumption in the United States
- 8. Figure 2 Per Capita Spending on Children and the Elderly in the United States Source: Issacs, 2009 124 journal of law, medicine & ethics S Y M P O S I U M Health Spending across Populations A substantial part of cross-generational transfers, especially in developed countries, are attributable to spending for education and health care. Figure 2 shows estimates of resources used in the United States in a typi- cal year by or for a “child” (up to age 18) and “elder” (over 65). Although there is a large disparity between the resources expended on the two groups, there is nothing inherently wrong, unethical, or amoral about the greater spending for our elders. Rather, it is a reflection of our collec- tive decisions on the amount of resources we chose to reallocate largely from the working population to those who are on both ends of life. As a society, we provide education for our children, and income and health care for the elderly. Unfortunately, the tradeoff between the two is not often analyzed.1 With fixed resources, at any point in time the more we
- 9. spend on one, the less we have to spend on the other — or the less workers have to consume. Currently in the U.S., most of the public transfers to the elderly occur at the national level, through the federal budget, while many of the decisions on education spending are made at the state and local levels. One exception to this general division of responsi- bility is Medicaid, which provides health care to parts of the lower-income population, including the dis- abled and elderly, and is funded by both the federal (55%) and state (45%) governments. Medicaid allows states some discretion as to whom they cover and how they deliver services, but dictates a minimum level of benefits. An expansion of the Medicaid program, by an additional 15 million people, is one of the ways last year’s health reform legislation provides coverage to the uninsured. This program, along with health spending for pub- lic employees and retirees, is putting increasing pres- sure on other state spending, particularly funding for education, which the states in turn are reducing and pushing down to the local level. While localities do not have to fund Medicaid, they do have health costs for employees and retirees putting similar pressure on education and other local responsibilities. Before reaching any inherently subjective conclu- sions, such as how much is “enough,” it is important to understand more about what health spending buys, and for whom. Figure 3 illustrates a perhaps obvious point that hospitals and physicians make up the majority of costs, and when lab work and other related services
- 10. are added, nearly 60% of the total. What may be more surprising is how relatively little is spent on some sec- tors, such as prescriptions and public health. Over time there has been a dramatic shift away from private financing of health care (insurance and out- of-pocket) to financing by and through government. Last year private insurance covered only about 1/3 of all spending, and out-of-pocket costs to patients amounted to 12% of the total. Most of this spending in any given year is incurred on behalf of a relatively small proportion of the popu- lation. Standard rules-of-thumb — 5% of the popula- tion spend 50% of the costs; 20% of the population make up 80% of the costs — suggest how concentrated health care needs are. In Figure 4, these “expensive” patients appear in the right-hand side of the graph. Included here are episodic expenses for maternity, a case of pneumonia, or trauma from an accident. Yet the vast majority, 75%, of spending in this right-hand side of the graph is for patients with chronic disease. High Cost of Health Care Is Due to Chronic Disease, Not the End of Life Advances in the prevention and treatment of infec- tious disease, the widespread adoption of water treat- ment in developed countries, the ability to diagnose and treat chronic illness, and the decline in smoking, have all contributed to an increase in the number of years we can expect to live. As we live longer, however, we tend to develop chronic disease, and often several chronic illnesses concurrently. For example, the “average” Medicare
- 11. Figure 3 The Composition of Health Care Spending in 2009 cost and end-of-life care • summer 2011 125 Crippen and Barnato patient in the top quarter of spending has five chronic conditions, sees 12 separate physicians over the course of a year, fills 50 prescriptions for various drugs, and is hospitalized at least once. For some, this treatment occurs at the end of their lives. About 27% of all Medi- care spending is used each year for people who die, a proportion that has been stable over several decades.2 The stability of this concentration suggests that what- ever is affecting overall cost increases is affecting dece- dents and survivors alike. It is not increases in end- of-life spending that is driving up the cost of health care, but overall health care costs propelled by the increase in chronic disease, technology to detect and treat it, and in the costs of treating patients with mul- tiple chronic conditions.3 In Medicare, most expensive patients live on for several years, and incur high costs such as repeat hospitalizations in subsequent years. It is not just the elderly who develop chronic dis- ease. Increasingly, children are developing diabetes and associated conditions, often due to obesity. More asthma is being diagnosed. Patients with addiction and behavioral health issues, including depression, often have chronic illnesses and are expensive to
- 12. treat. In fact, behavioral health issues are prevalent enough throughout all age groups that it will be dif- ficult to control costs without adequately addressing behavioral health as a co-morbidity. Figure 5 attempts to separate spending for typical chronic conditions by behavioral health diagnoses. This Medicaid popula- tion (which is undoubtedly more prone to issues of mental health and addiction), suggests the number of hospitalizations in a year may be 3-6 times more for patients with behavioral health complications, result- ing in as much as a $30,000 difference in the annual cost of treatment. Ultimately it is the complexity of treatment of multi- ple diseases, and our inability to treat complex patients satisfactorily with current practices, that is driving health spending on chronic disease. Dr. Gerard Anderson, updating some of his previous work on the nature of chronic disease in America, recently concluded: Unfortunately, while our health care needs have evolved, often the health care system has not. It remains an amalgam of past efforts to treat infec- tious diseases and acute illnesses. It does not focus on today’s current and growing problem — increasing numbers of people with chronic condi- tions, especially those with multiple chronic conditions…. Many people
- 13. with chronic conditions have multiple chronic conditions and this neces- sitates multiple caregivers. The cur- rent system provides few incentives for physicians and other caregivers to coordinate care across providers and service settings. We know that many people with chronic conditions report receiving conflicting advice from differ- ent physicians and differing diagnoses for the same set of symptoms. Drug-to- drug interactions are common, some- Figure 4 Per Capita Health Spending as a Percent of the Population It is not increases in end-of-life spending that is driving up the cost of health care, but overall health care costs propelled by the increase in chronic disease, technology to detect and treat it, and in the costs of treating patients with multiple chronic conditions. 126 journal of law, medicine & ethics S Y M P O S I U M times resulting in unnecessary hospi- talizations and even death. People with chronic conditions are getting services, but those services are not necessarily coordinated with one another, and they are not always the services needed to
- 14. maintain health and functioning.4 As exemplified by the expensive Medicare patients cited above, the dozen doctors delivering care are an assortment of largely specialists who are trained to treat specific diseases. The coordination of care, where it occurs often falls to general practitioners and inter- nists, who are paid less and who often do not have even the basic information from all the providers. Bet- ter health information systems will help this task, but it is far from sufficient to ensure success. More important is the development of more knowl- edge about how to treat multiple conditions in one patient. Dr. Cynthia Boyd of Johns Hopkins Univer- sity5 compared the recommended treatment for an elderly woman with five typical conditions for a female of her age: diabetes, hypertension, arthritis, osteopo- rosis, and difficulty in breathing (COPD). Applying the best-evidence medicine for each of the five conditions resulted in a large pharmacy load (12 medications, 20 pills a day), contradictory exercise regimes, and con- flicting dietary advice. Dr. Boyd concluded: Although CPGs (Clinical Practice Guidelines) provide detailed guidance for managing single diseases, they fail to address the needs of older patients with complex co-morbid illness…. It is evi- dent that CPGs, designed largely by specialty-dom- inated committees for managing single diseases, provide clinicians little guidance about caring for older patients with multiple chronic diseases.6 The Department of Health and Human Services has begun to recognize this challenge and issued a report in December 2010, entitled, New Strategic Framework
- 15. on Multiple Chronic Conditions.7 Health Spending across Generations Thus far we have considered how current spending for health care could crowd-out spending for other needs across the country, looking particularly at allo- cations for children. Again, it is not self-evident that the current allocation between the young, workers, and retirees is somehow wrong or unethical. Rather, it is demonstrative that the high cost of health care, if it could be reduced, could free up resources to be used for the young, to reduce public deficits, or returned to taxpayers. It is possible to examine how the current distribu- tion of resources will be affected in the future. Current deficits, to the extent they continue, will push more of the funding for today’s federal programs into the Figure 5 Hospitalizations for a Medicaid Population, by Disease and Behavioral Health Status Source: Center for Health Care Strategies cost and end-of-life care • summer 2011 127 Crippen and Barnato future, leaving interest and principal payments for generations to come. Figure 6 depicts the finances of the federal gov- ernment over a long period, wherein total revenues
- 16. amounted to about 18% of the economy (GDP) and spending around 20% of GDP. In the last two years, revenues have fallen and spending has increased by historic amounts, resulting in deficits of 9-10% of GDP. Perhaps more important, the outlook for the future, while improved, is the continuation of large deficits. Revenues do increase over time (this graph assumes the Bush-era tax cuts are not made permanent) and spending declines somewhat before the impending retirement of the baby boom generation begins to push retirement and health spending up rapidly. In perhaps more understandable terms, the federal government currently spends the equivalent of roughly $30,000 per household in the United States, collects $20,000, and borrows $10,000. The $10,000 in new debt will be added to the $90,000 per household in previous borrowing. Interest payments on the debt amount to about $2,000 of the $30,000 in spend- ing. With the continued deficits in the current budget, interest payments will rise to $8,000 per household by 2020, just a few years from now. These numbers all pale in comparison to the approximately $750,000 per household in unfunded future promises — prom- ises made mostly for pensions and health care. The $10,000 for each household in new debt this year covers the deficit for the entire federal budget, not just spending for health care. In that sense, the borrowing could be attributed to any, or all, federal programs, including the wars in the Middle East. However, the ever-increasing health care costs in the budget, propelled by the retirement of the baby- boomers, will require very significant tax increases,
- 17. cuts in other programs, or continued unprecedented borrowing. Figure 7 suggests that these three federal programs for retirees and disabled will, in less than 20 years, require funding levels near the entirety of what we currently collect in federal revenues. Tax increases to cover these programs (while maintaining the rest of the budget) would amount to 4-5 times the size of the Bush-era tax cuts. These additional taxes would have to come largely from workers, rich and poor alike, to cover the gap. Borrowing to fill the hole would require yearly debt increases in the 100s of billions of dollars — amounts that our creditors around the world may, at some point, be reluctant to provide. Without conjecturing how this might all work out, it is fairly clear that increasing health care spending, particularly for the elderly baby boomers, on a scale promised under current law will likely result in at least some increased borrowing (along with tax increases and spending cuts in other programs). To the extent it does, future generations will be paying for the boom- Figure 6 Federal Revenues and Spending as a Percent of GDP 128 journal of law, medicine & ethics S Y M P O S I U M ers’ retirement, not just the boomers’ children as the basic social compact would suggest.
- 18. State and local governments, already under extreme financial pressures, will fare no better. As noted earlier, some states are approaching the time when spend- ing on health care will overtake that for education. In the future, sometime before mid-century, health care spending will exceed all other state spending. The current disparity between young and old will be greatly exacerbated and for those states who manage to borrow, the onus on future generations will be even larger. (A Word about) Health Reform With the passage of health reform legislation last year, there is the prospect of change in the patterns iden- tified earlier. The primary objective of the legislation is to expand financing and coverage of health care for previously uninsured citizens. On that score, if the legislation is successfully imple- mented, as many as 30 million more Americans will have some form of health coverage starting in 2014. It should not be surprising that this coverage will come at a substantial cost since giving more people more health care is the intent. The short-term debate is over whether tax increases and spending cuts in the leg- islation will be enough to cover these increased costs. The longer-term issue, however, is whether other changes — in payment systems, additional research on what works, and more decision making outside normal congressional pro- cesses — will help hold down future
- 19. cost increases. Skeptics abound and even proponents admit it will be years before we know how effective these changes can be. It is particularly uncertain that any of the changes will alter health care delivery, and there- fore costs, for the 75% of spending devoted to chronic care. Suffice it to say, rapidly growing health care costs will be a major concern and public issue for at least the next decade, and likely much longer. One case study is the State of Massa- chusetts. In 2006, Massachusetts enacted sweeping health care reform similar to that passed by the Congress earlier this year. In many fundamental ways, Massachusetts was a model for the federal legislation. The reforms are also similar in that Massachu- setts was successful in providing coverage for many more of its uninsured citizens. Costs, how- ever, have gone up considerably — much more than anticipated when the legislation passed — to the point where total for health care spending is 40% of the entire budget, almost twice that for education. Conclusion A large disparity exists between resources consumed by today’s children relative to their retired counter- parts. A considerable amount of the difference can be attributed to spending on health care. To the extent a question of ethics arises, it may come down to whether we are spending “enough” on our children to support
- 20. them in their youth and prepare them for the future. This disparity will grow over the foreseeable future and, based on current law and experience, cause more debt to be accumulated for upcoming generations to pay. We are financing some of today’s spending on health care by effectively borrowing from future gen- erations. We will likely do so in ever-larger amounts in the future. The ethics of foisting off the payment for our health consumption on unborn citizens provokes a sharper dilemma. Figure 7 Spending for Social Security, Medicare and Medicaid as a Percent of GDP Unless we change the practice of medicine and reduce future costs, and explicitly address the ethical dilemmas we face, there may come a time when our kids simply cannot afford us. cost and end-of-life care • summer 2011 129 Crippen and Barnato In both cases — allocation of resources across our current population and the practice of borrowing from future generations to fund current consumption — health care plays a major role. While end-of-life spending is significant, and any reduction would help ease both cases, it is the ongoing health care of citizens with multiple chronic conditions that poses the great- est challenge in resolving these dilemmas, for current
- 21. and future generations. The good news is that it is possible to give patients with chronic disease better health, and thereby reduce costs, by (among others): emphasizing, and paying for, coordination of care; recognizing the role behavioral health plays in physical health; and increasing patient compliance with treatment protocols. In addition, a national research agenda should be developed and funded to better understand the interactions of chronic conditions and their treatment, including pharmacy, and the role of patients in developing and implement- ing disease management. Unless we change the prac- tice of medicine and reduce future costs, and explicitly address the ethical dilemmas we face, there may come a time when our kids simply cannot afford us. FIGURE LEGENDS Figure 1. Life-Cycle Income and Consumption for the United States Over the course of a lifetime, there are distinct periods where we consume more than we produce (as children and retirees) and periods where we produce more than we consume (as working-age adults). The patterns vary by country, economy, and culture, and are reflective of the public programs in place to redistribute income from current workers to those too young or old to work. Figure 2. Per Capita Spending on Children and the Elderly (by Type of Spending in the United States) In the U.S., we provide much more support to our indi- vidual retirees than we do our children. The single most important reason for the difference is the dispar- ity of spending on health care. Figure 3. The Composition of Health Care Spend-
- 22. ing in 2009 National surveys allow estimates of the breakdown of health care dollars among the various providers of care, and other systemic costs such as public health. Figure 4. Per Capita Health Spending as a Percent of the Population There is not much validity to citing an “average” patient. While there are certainly people in the middle, there are essentially two groups of patients: those who don’t spend much in any given year, and those who spend a lot. The general rules of thumb are: 5% of the population drives 50% of total spending in a year; 20% of the population drive 80% of total costs. The mirror image is important for policy as well — 80% of the population spends only 20% of the total costs. Figure 5. Hospitalization for a Medicaid Population, by Disease and Behavioral Health Status Health care costs are often characterized as the expenses for treating physical maladies. However, those physical health costs, especially those for chronic care, are often compounded by behavioral health problems, such as depression or addiction. For this population it is not the cost of dying that drives costs as much as the cost of living. Figure 6. Federal Revenue and Spending as a Per- cent of GDP Figure 6 illustrates a number of points, but for these purposes perhaps the most important is that even after post-recession revenues recover (to nearly historic highs) and stimulus spending disap- pears, there is a substantial and growing gap between the two, resulting in large deficits that continue for decades. Figure 7. Spending for Social Security, Medicare and
- 23. Medicaid as a Percent of GDP These three programs, driven by retirement of the baby boomers and the ever-increasing cost of health care, will require nearly all the federal revenues collected in 2030. References 1. J. B. Isaacs, Public Spending on Children and the Elderly From a Life-Cycle Perspective, Brookings Institution, Washington, D.C., November 2009. 2. C. Hogan, J. Lunney, J. Gabel, and J. Lynn, “Medicare Ben- eficiaries’ Costs of Care in the Last Year of Life,” Health Affairs 20, no. 4 (July 2001): 188-195. 3. A. E. Barnato, M. B. Mcclellan, C. R. Kagay, and A. M. Garber, “Trends in Inpatient Treatment Intensity among Medicare Benefi- ciaries at the End of Life,” Health Services Research 39, no. 2 (April 2004): 363-376. 4. G. Anderson, Chronic Conditions: Making the Case for Ongo- ing Care, Johns Hopkins University, November 2007, at 5-6. 5. C. M. Boyd, J. Darer, C. Boult, L. P. Fried, L. Boult, and A. W. Wu, “Clinical Practice Guidelines and Quality of Care for Older Patients with Multiple Comorbid Diseases,” JAMA 294, no. 6 (2005): 716-724. 6. Id., at 720. 7. Department of Health and Human Services, New Strategic
- 24. Framework on Multiple Chronic Conditions, December 2010. Copyright of Journal of Law, Medicine & Ethics is the property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Nursing Priorities, Actions, and Regrets for Ethical Situations in Clinical Practice Pavlish, Carol, PhD, RN, FAAN;Brown-Saltzman, Katherine, MA, RN;Hersh, Mary, MSN, RN, CHPN, FPCN;... Journal of Nursing Scholarship; Dec 2011; 43, 4; ProQuest pg. 385 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further
- 25. reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
- 26. Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. International Journal of Nursing Studies 47 (2010) 635–650 Review Nurses’ ethical reasoning and behaviour: A literature review Sabine Goethals a,*, Chris Gastmans b, Bernadette Dierckx de Casterlé c a Catholic University College Ghent, Department of Nursing, Hospitaalstraat 23, 9100 Sint-Niklaas, Belgium b Centre for Biomedical Ethics and Law, Faculty of Medicine, Catholic University Leuven, Belgium c Centre of Health Services and Nursing Research, Catholic University Leuven, Belgium A R T I C L E I N F O Article history: Received 16 July 2009 Received in revised form 4 November 2009 Accepted 18 December 2009 Keywords:
- 27. Ethical behaviour Ethical decision making Ethical reasoning Ethics Nursing Literature review A B S T R A C T Background: Today’s healthcare system requires that nurses have strong medical– technical competences and the ability to focus on the ethical dimension of care. For nurses, coping with the ethical dimension of care in practise is very difficult. Often nurses cannot act according to their own personal values and norms. This generates internal moral distress, which has a negative impact on both nurses and patients. Objectives: The objective of this review is a thorough analysis of the literature about nurses’ ethical practise particularly with regard to their processes of ethical reasoning and decision making and implementation of those decisions in
- 28. practise. Design: We conducted an extensive search of the electronic databases Medline, Embase, Cinahl, and PsycInfo for papers published between January 1988 and September 2008. A broad range of search keywords was used. The 39 selected articles had a quantitative, qualitative, or mixed-method design. Findings: Despite the conceptual difficulties that the literature on the ethical practise of nurses suffers, in this review we understand nurses’ ethical practise a complex process of reasoning, decision making, and implementation of the decision in practise. The process of decision making is more than a pure cognitive process; it is influenced by personal and contextual factors. The difficulties nurses encounter in their ethical conduct are linked to their difficult work environment. As a result, nurses often capitulate to the decisions made by others, which results in a conformist way of acting and less individually adapted care. Conclusions: This review provides us with a more nuanced understanding of the way nurses
- 29. reason and act in ethically difficult situations than emerged previously. If we want to support nurses in their ethical care and if we want to help them to change their conformist practises, more research is needed. Especially needed are in-depth qualitative studies that explore the experiences of nurses. Such studies could help us better understand not only how nurses reason and behave in practise but also the relationship between these two processes. � 2010 Elsevier Ltd. All rights reserved. Contents lists available at ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns What is already known about this topic? � T 00 do he ethical dimension of care is difficult to realise in the complex and stressful work environment that charac- terizes today’s nursing practise. � N urses are regularly confronted with ethical decisions
- 30. that others make and that are in conflict with their own * Corresponding author. Tel.: +32 37808905; fax: +32 37663462. E-mail address: [email protected] (S. Goethals). 20-7489/$ – see front matter � 2010 Elsevier Ltd. All rights reserved. i:10.1016/j.ijnurstu.2009.12.010 personal values and norms. � N urses who cannot sufficiently integrate their own values and norms into their daily practise may experi- ence moral distress. Moral distress results in less appropriate patient care and in nurses’ burnout. What this paper adds � T his review provides a more nuanced understanding of the way nurses reason and act in ethically difficult situations. � mailto:[email protected] http://www.sciencedirect.com/science/journal/00207489 http://dx.doi.org/10.1016/j.ijnurstu.2009.12.010 S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650636 The process of decision making is more than a pure cognitive process; it is a difficult and complex process
- 31. influenced by personal and contextual factors. � T he difficulties nurses encounter in their ethical practise are linked to their difficult work environment. 1. Introduction Today, nurses’ practise is characterized by a strong emphasis on high technological interventions and financial limitations, and is dominated by economic values (Dean, 1998; Spitzer, 1998; Milisen et al., 2006). Nurses are therefore confronted with complex care situations in which they are expected to autonomously make decisions in delivering good care to patients and to do so within the confines of strict deadlines. ‘Good care’ is oriented towards the promotion of the patient’s well-being in its entirety, i.e., considering patients’ physical as well as psychological, relational, social, moral, and spiritual well-being and so can be considered as a moral practise (Gastmans et al., 1998). The ethical dimension of care cannot be restricted to specific ethical dilemmas in the context of the beginning and end of life. On the contrary, the ethical dimension of care is an essential part of nursing practise (Bishop and Scudder, 1990). Nurses make daily decisions that are ethically informed. Examples can be found in how they deal with intimacy and privacy (Mattiasson and Hemberg, 1998) and the use of physical restraints in their care for the elderly (Gastmans and Milisen, 2006). Acting responsibly in these and comparable situations requires not only medical/technical competency but also the ability to
- 32. reflect critically about ethical dilemmas and the ability to surpass the mere implementation of previously defined rules (Bolmsjö et al., 2006). Even though ethics is a constitutive element in current nursing education, research reveals that nurses face considerable difficulties when they have to implement the ethical dimensions of care in daily professional practise (Woods, 2005). Siebens et al. (2006) reported that nurses working in a complex work environment give priority to medical/technical interventions; establishing caring rela- tionships with their patients is of secondary importance. It is worrisome that nurses complain that it is impossible for them to practise according to their own ethical values or to voice ethical issues within the team. Furthermore, although nurses are regularly confronted with healthcare decisions that they perceive as morally wrong, they are expected to execute those decisions (Gutteriez, 2005). Nurses may feel that their self-image and integrity is threatened, if they have to comply with unwritten rules and routines and if they are unable to act according to their professional ideals because of practical circumstances (Sorlie et al., 2003; Torjuul and Sorlie, 2006). Regularly confronting such situations can lead to moral distress (Kälvemark et al., 2004; Gutteriez, 2005; Torjuul and Sorlie, 2006). According to Jameton (1984), nurses experience moral distress when they judge a particular decision to be ethically correct but are unable to execute it because of situational factors. Nurses most commonly respond to moral distress by being less involved with patients and family members and by providing less personalized care (Gutteriez, 2005). As for nurses them- selves, moral distress may lead to decreased job satisfac- tion, increased staff turnover, health problems, and burnout, with nurses eventually leaving the profession (Gutteriez, 2005; Torjuul and Sorlie, 2006). Where Schluter
- 33. et al. (2008) report a (developing) relationship between moral distress of nurses and the organization’s ethical climate, Pauly et al. (2009) confirm this relationship, which would be negatively correlated. Given the significant consequences of moral distress for nurses as well as for patients, it is essential to identify and to fully understand what is currently known in literature about nurses’ ethical practise. This insight may help us provide guidance to nurses that can support them in the ethical dimension of care. 2. Review 2.1. Aim The objective of this review was to thoroughly examine the literature about nurses’ ethical reasoning process and nurses’ ethical behaviour. Ethical practise includes the reasoning process, the associated decisions, and the actual implementation of the ethical decisions (Dierckx de Casterlé et al., 1997). Ethical reasoning involves the cognitive process of reasoning, which leads to moral decision making (Ketefian, 1989; Omery, 1989). We view ethical behaviour as putting an ethical decision into practise (Dierckx de Casterlé et al., 1997). In this review, we specifically address the following research questions: (1) How do nurses reason when they are faced with an ethical decision? (2) How do nurses implement their ethical decisions in practise? 2.2. Review methodology This review was conducted by following the guidelines of the United Kingdom Centre for Reviews and Dissemina-
- 34. tion Guidelines on Systematic Reviews (Centre for Reviews and Dissemination, 2001). Articles were read, and relevant data were isolated, compared, and related. After consulta- tion with the other researchers (BD, CG), concepts and themes were identified (Dixon-Woods et al., 2006). 2.3. Search strategy We conducted an extensive search in the databases Medline, Embase, Cinahl, and PsycInfo for papers pub- lished between January 1988 and September 2008 on nurses’ ethical practise. This review follows the review of Ketefian (1989), who systematically searched the litera- ture from 1983 to 1987. The following keywords were used: ‘ethical reasoning’, ‘ethical decision making’, ‘moral reasoning’, ‘ethical practise’, ‘ethical action’, ‘ethical behavio(u)r’, ‘moral behavio(u)r’, ‘moral judgment’. Each of these terms was combined with the wildcard term ‘nurs*’ and ‘research’. This resulted in 6889 results. Titles and abstracts were screened, and studies were included if they met the S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650 637 following criteria: (1) empirical research published in Dutch, French, English, and German; and (2) research that dealt with the ethical reasoning and/or ethical behaviour of nurses. Publications were excluded if (1) the article concerned only student nurses, and (2) the studies were reviews or (3) doctoral dissertations. Reference lists of all articles were examined for additional publications not previously identified (Centre for Reviews and Dissemina- tion, 2001). Manual search of bibliographies of relevant
- 35. articles was done and ethics experts (BD, CG) suggested other pertinent articles. These procedures added no articles. Our search procedure resulted in 39 papers which we examined critically. 2.4. Search outcome The search strategy yielded 39 appropriate publications that described 38 separate studies (Tables 1–3). The articles from Lützen and Nordin (1993b, 1994) were derived from the same study; therefore, we considered these articles together as representing one study. Thirteen studies used a quantitative design (Table 1); eighteen used a qualitative design (Table 2); and seven used a mixed method (Table 3). Ethical reasoning was studied in 24 studies, most of which were qualitative studies. Ethical behaviour was studied in ten studies, in which researchers used both quantitative and qualitative research designs. Four studies described both ethical reasoning and ethical behaviour processes (Carpenter, 1991; Vogel Smith, 1996; Dierckx de Casterlé et al., 1997, 2008). Only one study examined the relationship between ethical reasoning and the implementation of ethical decisions in practise (Dierckx de Casterlé et al., 1997). The studies were conducted in ten different countries: USA (n = 14); Sweden (n = 9); Canada (n = 4); Australia (n = 2); and Belgium, Denmark, Greece, Korea, Mexico, and South Africa (n = 1 for each country). Three studies reported results from internationally conducted research (Davidson et al., 1990; Norberg et al., 1994; Dierckx de Casterlé et al., 2008). Most research settings consisted of a combination of several acute and/or chronic settings. In 24 studies, the sample consisted of only nurses. The remaining studies
- 36. consisted of nurses and/or nursing students and/or doctors and/or other healthcare workers. The combined research population consisted of about 4100 nurses, mainly women, between 20 and 65 years old, and with a nursing experience ranging from <1 year to 39 years. 2.5. Methodological features The methodological features of the included studies are summarized in Tables 1–3. Barring one study (Kim et al., 2007), all quantitative studies implemented a descriptive, correlational or comparative design. In the quantitative studies, the sample sizes varied from 63 to 1592 nurses. Response rates, when mentioned, varied from 20% to 84% (Table 1). The sampling methods were very diverse: random sampling (Kuhse et al., 1997; Dodd et al., 2004); stratified random sampling (Erlen and Sereika, 1997); purpose sampling (Dierckx de Casterlé et al., 1997; Penticuff and Walden, 2000); convenience sampling (Corley and Selig, 1994; Kyriacos, 1995; Raines, 2000); and randomized convenience sampling (Ham, 2004). In some studies, the sampling method was not mentioned (Garritson, 1988; Elder et al., 2003; Kim et al., 2007). In the qualitative studies, the sample sizes varied from 9 to 169 nurses (Table 2). In half of these studies, nurses were purposefully selected using specific criteria, such as ‘experienced and good’ (Jansson and Norberg, 1989, 1992; Davidson et al., 1990; Aström et al., 1993, 1995; Norberg et al., 1994); ‘competent and reflective’ (Lützen and Nordin, 1993a, 1994); ‘recommended by peers and supervisors’ (Lützen and Nordin, 1993b); and ‘thoughtful about ethical questions’ (Oberle and Hughes, 2001). In the mixed-method studies, the sample sizes varied from 20 to 149 nurses (Table 3). In the study of Norberg et
- 37. al. (1994), nurses were also selected using the criterion ‘experienced and good’. In three other studies, the sampling method was convenience sampling (Chally, 1995; Mattiasson and Andersson, 1995; Monterosso et al., 2005). Many of the studies lacked clear conceptualisation and operationalization of the terms ‘ethical reasoning’ and ‘ethical behaviour’, leading to the development and use of customised definitions. Some studies even failed to define the concepts of ‘ethical reasoning’ and ‘ethical behaviour’. Especially in studies that used quantitative and mixed methods, various theoretical frames and definitions were used to study ethical reasoning and ethical behaviour processes. Theories that were frequently referred to were the moral development theory by Kohlberg (1981), the four principles of biomedical ethics by Beauchamp and Childress (1979), the justice-care perspective by Gilligan (1982), and deontological and teleological approaches. The use of established measurement instruments, like the Nursing Dilemma Test (Crisham, 1981) and the Judgment about Nursing Dilemmas (Ketefian, 1981) was very limited. Most researchers developed their own instruments to measure ethical reasoning and behaviour, using vignettes, dilemmas, and/or questionnaires that measured variables considered to be connected with ethical reasoning and/or ethical behaviour. In some of the qualitative studies, nurses presented ethically difficult situations and then described how they subsequently handled these situations in practise (Erlen and Frost, 1991; Grundstein-Amado, 1992; Uden et al., 1992; Aström et al., 1993, 1995; Lützen and Nordin, 1993a,b, 1994; Chally, 1995; Oberle and Hughes, 2001; Rodney et al., 2002; Tsaloglidou et al., 2007). In sixteen
- 38. qualitative studies, respondents were interviewed. Two studies used focus groups. Only two studies combined two methods to obtain data (Rodney et al., 2002; Tsaloglidou et al., 2007). Many of the studies used well-known metho- dological approaches like the grounded theory (n = 4), phenomenology (n = 4), constructivist methodology (n = 2), and narrative theory (n = 1). 2.6. Quality appraisal One researcher (SG) assessed the included publications using the assessment sheets prepared and tested by Table 1 Quantitative studies included in the literature review. Author(s) Country Aim(s) of the study Design- sample Data collection Data analysis Care setting Response rate (RR) Garritson (1988) USA 29 psychiatric inpatient units in private, county, veterans administration university hospitals To investigate nurses’ ethical
- 39. decision-making patterns Quantitative 177 registered nurses (RNs) RR: 20–4% Questionnaires presented to nurses during staff meetings, distributed to nurses’ mailboxes Questionnaire included: staff demographic characteristics, case vignettes, nursing philosophy statement Frequency data Bowker Test of Symmetry Corley and Selig (1994) USA Federal teaching hospital
- 40. (850 beds)—all CCUs: medical, surgical, coronary, haemodialysis, emergency admitting To examine how often nurses use principled thinking to decide on actions in specific ethical situations Quantitative exploratory 91 RNs RR: 82% (n = 75) Questionnaire: Nursing Dilemma Test (NDT) (Crisham, 1981) Six client care dilemmas considering the following: nurses’ principled thinking, practical considerations,
- 41. and other issues considered in making a decision Frequency data t-test Pearson product moment correlation Kyriacos (1995) South Africa Convenience sample of nurses following an ethical workshop To explore nurses’ stage of thinking in moral judgment development 109 nurses RR: 63% (n = 69) Questionnaire: completing the questionnaire on a
- 42. one-day nursing ethics workshop NDT (Crisham, 1981) Six client care dilemmas—considering nurses’ principled thinking Frequency data Dierckx de Casterlé et al. (1997) Belgium 14 Flemish schools of nursing University students Expert nurses To explore nursing students’ ethical behaviour in five nursing dilemmas Quantitative descriptive correlational 2634 nursing students
- 43. (technical–professional) 176 university students 59 expert nurses Questionnaire: Ethical Behaviour Test (EBT) based on DIT (Rest, 1976) and NDT (Crisham, 1981) developed by Dierckx de Casterlé (1993) Five stories depicting nurses in daily ethical dilemmas were used to assess the subjects’ perceptions of the nursing dilemma and the way in which they would reason and act in that situation Two-way analysis of variance Bonferroni method Multivariate analysis (MANOVA)
- 44. Erlen and Sereika (1997) USA 2 tertiary care university-affiliated hospitals 16 ICUs To measure ethical decision making and stress To examine the relationship of selected nurse characteristics with aspects of ethical decision making and stress To examine the relationship between ethical decision-making and stress in ICU nurses Quantitative descriptive correlational
- 45. Stratified random sample—proportional allocation 80 nurses RR: 78.8% (n = 63) Questionnaires mailed to interested nurses NEDM-ICU: Nursing Ethical Decision Making—ICU included: NEDM-ICU part I, WPR: workplace restrictions, RT: risk taking. NEDM-ICU part II, NA: nurse autonomy, PR: patient rights, RTR: rejection traditional role, HPSI: Health Professional Stress Inventory 30 general stressful situations—identification of how stressful nurses perceive a
- 46. particular situation Pearson product moment correlation Student’s t-test One-way analysis of variance (ANOVA) Tukey’s pairwise multiple comparison Mann–Whitney U test Spearman’s rank order correlation S . G o e th a ls e t
- 48. ie s 4 7 (2 0 1 0 ) 6 3 5 – 6 5 0 6 3 8 Kuhse et al. (1997) USA Victorian and New South Wales Medical
- 49. Boards Australian Nursing Federation To discover whether gender or occupation affected the approach (partialist or impartialist) that participants took in response to various moral dilemmas Quantitative descriptive correlational Random sample 400 doctors from Victoria, 200 doctors and 400 nurses form New South Wales RR: 30.5% (n = 122 nurses) Questionnaire mailed to a randomly selected sample of nurses and doctors
- 50. Questionnaire included: 4 moral dilemmas involving combinations of (healthcare) professional, non-professional, life-threatening, and non-life-threatening situations Lambda measures Penticuff and Walden (2000) USA 4 obstetrics units and 4 neonatal ICU from 5 major hospitals To explore the relative contributions of practical environment characteristics and nurses’ personal and professional characteristics
- 51. on the willingness of perinatal nurses to be involved in activities used to resolve clinical ethical dilemmas Quantitative descriptive correlational Purpose sample 200 nurses RR: 64% (n = 127) Questionnaires: personal invitation to nurses—nurses who agreed received questionnaires Questionnaire included: Demographic Data Sheet, PVQ: Perinatal Value Questionnaire, NEIS: Nursing Ethical Involvement Scale Multiple regression analysis
- 52. Raines (2000) USA Oncology nurses To determine the relationship between moral reasoning, coping style, and ethics stress Quantitative descriptive correlational—survey Convenience sample 795 nurses RR: 29% (n = 229) Questionnaires to oncology nurses members of Oncology Nursing Society (nationwide), a professional nursing organization Questionnaire included: Demographic Data Sheet, MRQ: Moral Reasoning Questionnaire, WCI: ways of coping inventory, ESS:
- 53. Ethical Stress Scale, EIS: Ethics Inventory Instrument Descriptive statistics Multiple regression analysis Analysis of variance (ANOVA) Elder et al. (2003) Australia-Queensland Hospital environment To explore differences in the ethical attitudes of medical students and nurses Quantitative descriptive Voluntary participation 125 medical students 67 nurses Questionnaire was completed by nurses during a seminar
- 54. Questionnaire containing 23 vignettes followed by four alternative responses t-test Analysis of variance (ANOVA) Dodd et al. (2004) USA, New York 3 urban hospitals A non-profit hospital (903 beds) A university hospital (600 beds) A rehabilitation hospital (396 beds) To explore the extent to which nurses engage in ethical activism and ethical assertiveness Quantitative descriptive
- 55. correlational Random sample 165 nurses from 3 hospitals RR from 3 hospitals: 26–41% Postal self-administered 72-item questionnaire Ethical activism Ethical assertiveness Analysis of variance (ANOVA) Bonferroni post hoc analysis t-test Multiple regression analysis Ham (2004) USA 4 Midwestern states To study the effects of
- 56. environmental influences and previous ethical decision-making experiences on nurses’ moral reasoning Quantitative descriptive Randomized convenience sample 200 nursing students 500 RN RR RN: 24% (n = 120) Questionnaire mailed to randomly selected nurses in the four-state area NDT (Crisham, 1981) Six client care dilemmas—considering nurses principled thinking and practical considerations Pearson product moment correlation
- 57. One-way analysis of variance Kim et al. (2007) Korea Hospital environment To examine changes in nursing students’ moral judgment after becoming qualified nurses Quantitative descriptive 100 nursing students 80 nurses Questionnaire JAND: Judgment about Nursing Dilemma (Ketefian, 1981) modified to a Korean population (Kim, 1999) Idealistic—realistic decision making Paired t-test Independent t-test
- 81. t re g re ss io n a n a ly si s S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650640 Hawker et al. (2002). This screening method enabled us to evaluate the quality of both quantitative and qualitative studies. We analysed the 38 studies on a number of aspects, including method and analysis, ethical issues, quality and strength of evidence, and their relevance to the research question. With this system, it was possible to calculate a summed score (9 = very poor; 36 = good), reflecting the methodological strength of the studies. The minimum score was 19/36 and the maximum score was 33/36. In addition, the articles were assessed on the criteria of validity, reliability (for the quantitative studies), and the criteria of trustworthiness (for the qualitative studies) (Polit and Beck, 2008).
- 82. The shortcomings of the quantitative studies mostly were related to issues of confidentiality, sensitivity, and consent. Most of the quantitative studies discussed the reliability and validity of the instruments only to a limited extent. The authors of these studies most often limited themselves to a description of the development of the instruments and to a report of internal consistency scores. An obvious shortcoming of most of the qualitative studies was a rather limited description of the samples, the methods of data collection, and data analysis. Little attention was spent on reflexivity and possible bias; however, most authors did use a number of methods to enhance the trustworthiness of their studies. All inter- views were audiotaped and transcribed. Most used one method for data collection, while Rodney et al. (2002) used focus groups and open-ended questions. Tsaloglidou et al. (2007) applied interviews and participant observation techniques to collect data. Several researchers used investigator triangulation for their analyses (Jansson and Norberg, 1989, 1992; Carpenter, 1991; Erlen and Frost, 1991; Grundstein-Amado, 1992; Uden et al., 1992; Aström et al., 1993; Norberg and Uden, 1995; Vogel Smith, 1996; Varcoe et al., 2004; Monterosso et al., 2005). In addition, member-checking and the audit trail under the form of field notes, logs, and theoretical memos were used (Lützen and Nordin, 1994; Oberle and Hughes, 2001; Rodney et al., 2002; Tsaloglidou et al., 2007). Only two studies men- tioned that saturation was reached (Carpenter, 1991; Uden et al., 1992). 3. Findings The ethical practise of nurses is a complex process that combines the processes of ethical reasoning and ethical behaviour (Vogel Smith, 1996; Dierckx de Casterlé et al.,
- 83. 1997, 2008). The study of Vogel Smith (1996) labelled the inter-related processes of ethical reasoning and ethical conduct ‘deliberation’ and ‘integration’, respectively. Deliberation or the process of reasoning by nurses involves the consideration of the different factors that affect ethical decision making. Integration concerns the implementation of nurses’ decisions in clinical practise. Personal and contextual factors play an essential role in both processes. Examples of personal factors are nurses’ values, convic- tions, experiences, knowledge, and skills. Contextual factors include opinions and expectations of other nurses, doctors, and family. They also include rules and routines, and procedures and guidelines that are specific to wards in Table 2 Qualitative studies included in the literature review. Author(s) Country Aim(s) of the study Sample Data collection Data analysis Jansson and Norberg (1989) Sweden Oncological, medical, surgical clinics To elucidate ethical reasoning of experienced nurses concerning the
- 84. feeding of terminally ill cancer patients 20 RN ‘good and experienced’ Structured interviews Qualitative analysis Coding scheme Independent coding Davidson et al. (1990) Canada, USA, Switzerland, Finland, Sweden, Australia, China, Israel Variety of acute care centres To compare the ethical reasoning of nurses associated with the feeding of terminally ill elderly cancer patients 169 nurses in 8 countries ‘good and experienced’ Structured interviews Qualitative analysis
- 85. Coding scheme Carpenter (1991) USA 5 private agencies or hospitals 6 work settings affiliated with the Roman Catholic church 9 agencies publicly owned To examine the ethical decision-making processes of psychiatric nurses in clinical practise 20 RNs who had worked at least 1 year in a psychiatric setting Open-ended interviews Qualitative analysis Thematic analysis Erlen and Frost (1991) USA Medical–surgical Critical care setting
- 86. Psychiatric Hospital To examine how nurses’ experiences influence ethical decisions related to patient care management Convenience sample 25 nurses In-depth interviews using perceptions of nursing ethics interview schedule Content analysis Independent coding Grundstein-Amado (1992) Canada Nurses Acute-care setting Long-term care setting
- 87. Doctors Family practise Internal medicine Long-term care To assess differences in the ethical decision-making of nurses and doctors 9 nurses 9 doctors In-depth, semi-structured interviews Qualitative analysis Jansson and Norberg (1992) Sweden Nursing home Psychogeriatric clinic Somatic long-term clinic
- 88. To elucidate ethical reasoning of experienced nurses working in dementia care 20 nurses 8 head nurses 12 staff nurses ‘experienced and good’ Structured interviews Qualitative analysis Coding scheme Independent coding Uden et al. (1992) Sweden Department of internal medicine in an oncology university hospital To examine the ethical reasoning in nurses and physicians Convenience sample 23 nurses 9 physicians
- 89. Interviews: narrations of any ethically problematic care situation experienced Qualitative analysis Independent coding Narrative theory Lützen and Nordin (1993a) Sweden Various psychiatric settings To conceptualise the experiential aspect of moral decision-making Purpose sample 14 nurses (>5 years experience) ‘recommended by peers and supervisors’
- 90. In-depth interviews Qualitative analysis Grounded theory (Glaser and Strauss, 1967; Corbin and Strauss, 1990) Contextual research approach Ethnograph for first and second levels of analysis Lützen and Nordin (1993b) Sweden Hospital setting Community clinic To study the moral decision-making experiences of nurses working in a psychiatric nursing setting 14 nurses (>5 years experience)
- 91. ‘competent and reflective’ In-depth interviews Qualitative analysis Grounded theory (Glaser and Strauss, 1967; Corbin and Strauss, 1990) Contextual research approach Ethnograph for first and second levels of analysis S . G o e th a ls e t a l./
- 93. 7 (2 0 1 0 ) 6 3 5 – 6 5 0 6 4 1 Table 2 (Continued ) Author(s) Country Aim(s) of the study Sample Data collection Data analysis Sherblom et al. (1993)
- 94. USA 3 hospitals in a large metropolitan area To describe nurses’ ethical concerns 31 female staff nurses Interviews Qualitative analysis Responsive reader method Lützen and Nordin (1994) Sweden Hospital setting Community clinic To study the moral decision-making experiences of nurses in psychiatric practise 14 nurses (>5 years experience) ‘competent and reflective’ Interviews Qualitative analysis Grounded theory
- 95. (Glaser and Strauss, 1967; Corbin and Strauss, 1990) Contextual research approach Ethnograph for first and second levels of analysis Aström et al. (1993) Sweden Hospital setting Oncological, medical and surgical clinics in Northern Sweden To examine the experiences of nurses in ethically difficult situations To define the expression ‘It depends on the situation at hand’ 18 nurses: 14 staff nurses and 4 ward nurses Interviews Qualitative analysis
- 96. Phenomenology— Hermeneutic Aström et al. (1995) Sweden Oncological, medical, and surgical clinics specialized in cancer care To explore how nurses manage ethically difficult care situations 14 staff nurses, 4 head nurses RR: 90% ‘experienced in the care of cancer patients’ Interviews Qualitative analysis Structural analysis Phenomenology— Hermeneutic Viens (1995) Mexico A variety of primary care
- 97. settings in a large city in the western United States To describe and analyse the process of moral reasoning 10 nurse practitioners Interviews Qualitative analysis Phenomenology Vogel Smith (1996) USA Medical–surgical, paediatrics, obstetrics, and psychiatric units, and various IC settings in one hospital To examine the experience of staff nurses in ethical decision-making Random sample 19 nurses Interviews Phenomenology Ethnograph program Giorgi’s method
- 98. (Giorgi et al., 1975) Oberle and Hughes (2001) Canada Adult medical–surgical units in one large hospital To examine similarities and differences in the ethical reasoning of doctors and nurses Nominated sample 14 staff nurses ‘‘thoughtful about ethical questions’, 7 doctors Unstructured interviews Qualitative analysis Grounded theory (Corbin and Strauss, 1990)
- 99. Thematic analysis Rodney et al. (2002) Canada Mid-sized metropolitan area with one health region Large metropolitan area with several health regions Settings: maternity, paediatrics, medicine, surgery, critical care, emergency, operating room, oncology, psychiatry, rehabilitation, long-term care, home care, and community care To examine the complexity of nurses’ ethical decision-making Theoretical sampling 19 focus groups: 3 groups advanced-practise nurses, 12 groups practising
- 100. nurses, 4 groups nursing students, 87 participants Focus groups Open-ended trigger questions Constructivist methodology (Lincoln and Guba, 1985) Varcoe et al. (2004) Canada 19 practise settings 10 different organizations To study the enactment of ethical practise in nursing 87 nurses, 41 nurses mid-sized metropolitan area, 46 nurses larger metropolitan area Focus groups Qualitative analysis Interpretive constructivist paradigm
- 101. Tsaloglidou et al. (2007) Greece 9-bed clinical nutrition unit—large teaching hospital in UK To determine nurses’ ethical decision-making role in artificial nutritional support 12 RN 2 consultants, 1 dietician Participant observation Semi-structured interviews Qualitative analysis Content analysis S . G o
- 104. 2 Table 3 Mixed-method studies included in the literature review. Author(s) Country Aim(s) of the study Design—sample Data collection Data analysis Care setting Response rate Martin (1989) USA, Texas Neonatal intensive care units (NICU) 5 large urban hospitals in the Southwest To determine nurses’ involvement in treatment decisions and factors influencing their participation in the decision-making process 83 RNs NEDMS: Nursing Ethical Decision Making Scale Semi-structured interviews
- 105. Frequency data Qualitative analysis Ethnograph for analysis Norberg et al. (1994) Sweden, USA, Australia, Canada, China, Finland, Israel Nurses from institutions providing high-quality care To compare the ethical reasoning of nurses in the feeding of a severely demented patient who seems to refuse food, this in a variety of cultures Structured interviews Ranking of the ethical principles
- 106. Coding scheme Chi-square test Chally (1995) USA 31-bed level III NICU Midwest Two 10-bed adult ICU Midwest To compare and contrast the perspective used by nurses working in neonatal and adult ICUs when making moral decisions Convenience sample 26 NICU nurses 25 adult ICU nurses Semi-structured interviews 12 open-ended interview questions Identification of Care and Justice Taxonomy Demographic variables
- 107. and perspective Interpretive method of analysis Chi-square test Norberg and Uden (1995) Sweden Geriatric and surgical care unit one large hospital To determine whether gender and different healthcare settings affect the content and form of moral reasoning 30 physicians 38 RNs 40 enrolled nurses (EN’s) Interviews Comparison between physicians, RNs, and
- 108. enrolled nurses concerning form and content of their moral reasoning Phenomenology—hermeneutic Chi-square test Mattiasson and Andersson (1995) Sweden 13 nursing homes in the county of Stockholm To explore ethical awareness: autonomous vs. heteronomous The following were assessed: nurses’ personal opinion of the case, unit’s anticipated decision regarding the case, responses analysed from the perspective of bioethical principles Convenience sample
- 109. 41 nurses 46 assistant nurses 83 nurse’ aides 17 other staff Self-report questionnaire: Hypothetical vignette about restraint Percentage per ethical principle for personal opinion and unit’s anticipated opinion Distribution of ethical awareness Content analysis Frequency data Holm et al. (1996) Denmark 5 internal medicine departments To assess the ethical reasoning content
- 110. of nurses and physicians in terms of style and time used by participants 21 physicians 20 nurses 7 Focus groups for content analysis Discussion style used Discussion time used Content analysis Sign test Fisher’s exact test Mann–Whitney U test Monterosso et al. (2005) Australia 2 NICUs of the sole perinatal tertiary referral centre of Western Australia
- 111. To explore to what extent nurses are involved in complex clinical and ethical decision-making Nurses’ understanding of patient advocacy in NICUs Categories of infants causing most concern in NICUs Convenience sample 200 nurses RR: 30% (n = 61) Nurses were invited to participate Questionnaire contains: DCSN: Decisions in Caring for Sick Newborn Infants Questionnaire Demographic characteristics Patient advocacy Nurses’ involvement in clinical
- 112. and ethical decision making Open-ended questions Descriptive statistics Thematic analysis S . G o e th a ls e t a l./ In te rn a tio n
- 114. 6 3 5 – 6 5 0 6 4 3 S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650644 which nurses work. Most of the studies analysed for this review support aspects of the findings of Vogel Smith (1996); therefore, we used their study as a guideline for structuring and integrating the different research results in this review. 3.1. Ethical reasoning Many of the studies endorsed the complexity of the reasoning process. From their ethical awareness, nurses observe, analyse, and judge a given problem in a specific care context. Nurses consider many factors that guide them in their eventual ethical decision making (Vogel Smith, 1996; Lützen and Nordin, 1993a; Carpenter, 1991; Viens, 1995; Rodney et al., 2002; Grundstein-Amado, 1992). They weigh various alternatives, make choices, and
- 115. make decisions (Grundstein-Amado, 1992; Lützen and Nordin, 1993a; Mattiasson and Andersson, 1995; Viens, 1995; Vogel Smith, 1996). To justify their decisions, they rely on medical knowledge, personal values and experi- ences, and the consequences of their possible choices (Grundstein-Amado, 1992). As a result, the ethical reason- ing process is embedded within the specific context and is determined by nurses within the context of the nurse– patient relationship. Here, given the important contextual embeddedness of nurses’ ethical reasoning and decision making, it cannot be reduced to its cognitive dimension. Ethical reasoning is studied from various perspectives. Grundstein-Amado (1992) and Holm et al. (1996) demon- strated that nurses reason using different theories and fundamental moral principles. They use deontological and teleological theories or a combination of both. Research into the ethical principles on which nurses ground their analysis shows that they apply various ethical principles, such as the principles of biomedical ethics, with a preference for beneficence and respect for autonomy (Garritson, 1988; Jansson and Norberg, 1989, 1992; Davidson et al., 1990; Norberg et al., 1994; Mattiasson and Andersson, 1995). They orient themselves from the perspective of the ethics of care or from the ethics of justice (Sherblom et al., 1993; Chally, 1995; Norberg and Uden, 1995; Kuhse et al., 1997). However, some authors emphasized that the principles and perspectives that are applied do not exclude each other, but that nurses integrate both care and justice perspectives in their decision-making processes (Sherblom et al., 1993; Chally, 1995). Both studies by Dierckx de Casterlé et al. (1997, 2008) indicated that nurses, when one applies the moral development stages from Kohlberg (1981), attribute more weight to conventional arguments (third and even fourth stage) than to post-conventional arguments (fifth and sixth stage).
- 116. Many of the studies that investigated ethical reasoning described the personal relationship between nurses and their patients. This caring relationship forms the context for the ethical assessment (Martin, 1989; Uden et al., 1992; Grundstein-Amado, 1992; Lützen and Nordin, 1993b, 1994; Chally, 1995; Viens, 1995; Vogel Smith, 1996; Oberle and Hughes, 2001; Rodney et al., 2002, Varcoe et al., 2004; Tsaloglidou et al., 2007). Driven by the ideal of care and with the aim of ‘doing good’ for the patient, nurses take the patient’s life history, feelings, wishes, intentions, and integrity into account (Jansson and Norberg, 1989; Grundstein-Amado, 1992; Lützen and Nordin, 1993b, 1994; Rodney et al., 2002). This finding is supported by various studies that indicated that a nurse’s ethical decision emerges as a result of the patient’s need for specific care, which is also influenced by the nurse’s relationship with the patient’s family and the team within the context of treatment and care (Jansson and Norberg, 1989, 1992; Davidson et al., 1990; Aström et al., 1993; Norberg et al., 1994; Viens, 1995; Vogel Smith, 1996; Rodney et al., 2002; Varcoe et al., 2004). As ethical reasoning is embedded in the personal relationship between a patient and a nurse, the patient’s and nurse’s personal qualities influence the ethical decision-making process. Nurses are strongly driven by values (Grundstein-Amado, 1992; Viens, 1995; Vogel Smith, 1996; Dierckx de Casterlé et al., 1997; Penticuff and Walden, 2000; Raines, 2000; Rodney et al., 2002; Varcoe et al., 2004; Monterosso et al., 2005): convictions, religion, education, and upbringing (Jansson and Norberg, 1992; Vogel Smith, 1996). In addition, nurses are inspired by their intuitions and feelings as they undertake ethical reflection (Lützen and Nordin, 1993a; Aström et al., 1995); and by their personal and professional experiences
- 117. (Jansson and Norberg, 1989, 1992; Uden et al., 1992; Grundstein-Amado, 1992; Viens, 1995; Vogel Smith, 1996; Erlen and Sereika, 1997; Varcoe et al., 2004; Monterosso et al., 2005). Some studies indicated that ethical reasoning is supported by medical and nursing knowledge and skills (Grundstein-Amado, 1992; Lützen and Nordin, 1993a; Vogel Smith, 1996; Varcoe et al., 2004; Tsaloglidou et al., 2007). Nurses’ ethical reasoning was also influenced by their collaboration with the patients’ family as well as with colleagues, doctors of the ward, and the institution (Jansson and Norberg, 1989, 1992). Nurses find it very important to share their ethical dilemmas with other nurses, to receive support, and to share their decisions with their colleagues (Uden et al., 1992; Aström et al., 1993; Raines, 2000). However, because nurses seek to adhere to the majority view of the nursing staff, they often put their own opinions aside (Jansson and Norberg, 1989, 1992; Davidson et al., 1990; Norberg et al., 1994). Different studies stated that nurses changed their decisions following a medical order (Jansson and Norberg, 1989, 1992; Davidson et al., 1990; Norberg et al., 1994). These situations can interfere with, influence, and change the development of nurses’ conclusions (Uden et al., 1992; Grundstein- Amado, 1992; Aström et al., 1993; Lützen and Nordin, 1994; Oberle and Hughes, 2001; Rodney et al., 2002). On the other hand, some elements facilitated ethical decision making: education, guidelines, standards, sup- portive colleagues (Rodney et al., 2002); and years of experience at the same job (Erlen and Sereika, 1997). Other factors hindered decision making: dominance within the medical profession, a stressful work environment with complex patient situations, insufficient resources, time,
- 118. and workload pressure (Oberle and Hughes, 2001; Rodney et al., 2002). Corley and Selig (1994), Kyriacos (1995), and Ham (2004) confirmed some of these impediments, S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650 645 reporting that experienced nurses in their ethical reason- ing give more importance to practical considerations, like time and means, and less weight to ethical principles. The studies of Rodney et al. (2002) and Varcoe et al. (2004) reported that nurses find a middle ground between their values and those of their colleagues and institution. These values often conflict with each other. Consequently, the decision-making process of nurses is not always straightforward and is characterized by a personal and professional struggle to realise what is good for the patient. Hereby nurses experience tension between their personal values, professional ideals, and the expectations of others (Lützen and Nordin, 1993a). Nurses experience an internal conflict when their personal values and professional responsibilities do not harmonize. This conflict can be manifested as tension between the ‘morally correct’ decision and the ‘legally correct’ decision (Lützen and Nordin, 1993b). How nurses cope with this tension may differ greatly. Rodney et al. (2002) reported that nurses looked for alternative solutions, like a wait-and-see approach or leaving the decision to others. The studies of Dierckx de Casterlé et al. (1997, 2008) reported that, in difficult situations, conventional arguments (Kohlberg’s third and even fourth stages), mostly influenced nurses’ decisions, indicating that their decisions were mostly influenced by professional norms, laws, and rules. Thus, nurses forsake their values and principles in order to adapt
- 119. to the opinions and expectations of others. There are also, however, nurses who place their values above professional expectations (Viens, 1995; Dierckx de Casterlé et al., 1997, 2008; Raines, 2000; Corley and Selig, 1994; Ham, 2004). In the studies of Raines (2000) and Corley and Selig (1994), 42.8% and 63% of nurses, respectively, took this approach. Moreover, the studies of Dierckx de Casterlé et al. (1997, 2008) observed that expert nurses, whose capacity for ethical acting in nursing dilemmas was estimated to be high, placed their values above professional expectations. Indeed, the reasoning of these nurses was not guided by the expectations of others or by the customs of their environment but was guided by their desire to provide the best patient care. 3.2. Ethical behaviour The ethical behaviour of nurses is a strong relational and contextual process in which personal and contextual aspects play an important role (Vogel Smith, 1996; Varcoe et al., 2004). In order for nurses to implement their decision in practise, it is important they are allowed to act as patient advocates. Additionally, consultation and a good relation- ship between the involved actors are essential for the process of integration. Having authority and power also contributes substantially to the implementation of ethical decisions in practise (Vogel Smith, 1996). Various studies, however, indicated that a gap exists between the ‘ideal’ ethical decision and the ‘real’ ethical behaviour (Sherblom et al., 1993; Raines, 2000; Kim et al., 2007). Some authors illustrated how nurses have difficul- ties in implementing their decisions in practise (Uden et al., 1992; Oberle and Hughes, 2001; Varcoe et al., 2004; Dierckx de Casterlé et al., 1997, 2008). Many of the studies
- 120. showed that contextual factors often limited nurses’ abilities to implement their decision in practise or to act according to their values and norms (Dierckx de Casterlé et al., 1997, 2008; Varcoe et al., 2004; Oberle and Hughes, 2001; Rodney et al., 2002; Uden et al., 1992; Erlen and Frost, 1991; Erlen and Sereika, 1997; Raines, 2000; Kim et al., 2007; Penticuff and Walden, 2000; Sherblom et al., 1993). Dierckx de Casterlé et al. (1997, 2008) reported that the chance that nurses actually implement their decisions becomes smaller when they are confronted with difficult contextual circumstances. In such situations, nurses often do not apply their decisions in practise but rather conform to existing practises and group ethics. Various studies showed that nurses are only indirectly, occasionally, or not at all involved in the ethical decision- making process (Martin, 1989; Monterosso et al., 2005; Tsaloglidou et al., 2007). As a result, they often do not feel personally responsible for their decisions, rather they feel that their role as patient advocates becomes lost (Martin, 1989; Uden et al., 1992; Monterosso et al., 2005). Nurses also experienced hierarchical relationships and traditional structures of power in the work environment as obstruc- tions, preventing them from acting ethically. Poor coopera- tion with doctors, not being able to discuss their ethical concerns, and a feeling of being ignored and not being respected in their professional abilities all created barriers that hindered nurses from acting on behalf of a patient’s best interest (Martin, 1989; Erlen and Frost, 1991; Chally, 1995; Tsaloglidou et al., 2007; Varcoe et al., 2004). These circumstances gave nurses the impression that they had little or no power to influence outcomes or the resolution of ethical dilemmas (Erlen and Frost, 1991; Penticuff and Walden, 2000). This often results in a reduced willingness to take action when ethical dilemmas arise. Nurses who are personally concerned about ethical dimensions and who
- 121. focus primarily on the morally relevant aspects of each patient’s situation are more likely to be involved in dilemma resolution activities (Penticuff and Walden, 2000). Varcoe et al. (2004) reported that nurses often find themselves lodged between the patient and the physician. Contrasting values and expectations often lead to tensions and conflicts in the provision of care, to which nurses respond in different ways. They do not react immediately in conflict situations but weigh the pros and cons. Various elements are taken into account, including the personality of the nurse, his or her position vis-à-vis the other actors, the importance of the situation, implicit and explicit customs of the institution, and the risk of negative repercussions. Carpenter (1991) stated that nurses could react in three different ways: They could directly address the person with whom they are in conflict; they could act indirectly; or they could do nothing. An example of reacting indirectly is discussing the conflict with a colleague, the head nurse, nursing staff, a social worker, or a physician (Martin, 1989; Raines, 2000; Penticuff and Walden, 2000). Some nurses, however, do succeed in going against deep-rooted routines, taking risks in order to act according to their own values and norms (Lützen and Nordin, 1993b; Viens, 1995). According to the results of Dierckx de Casterlé et al. (1997, 2008), expert nurses have a higher S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650646 chance of effectively implementing their ethical decisions in practise. They rely mostly on post-conventional argu- ments (Kohlberg’s fifth and sixth stage) to implement their
- 122. decisions. Martin (1989), Aström et al. (1995) and Varcoe et al. (2004) reported that knowledge, experience, risk taking, boldness, and strong problem-solving capabilities contribute to the fact that nurses eventually will act when confronted with ethical problems. Besides personal factors, contextual factors can also contribute to an active intervention when ethical problems occur. Being involved in ethical decision making, achieving a mandate in ethics deliberations, and being able to positively collaborate with physicians seem to prompt nurses to strive for the patient’s best interest (Dodd et al., 2004). Carpenter (1991), Erlen and Sereika (1997), and Raines (2000) reported that difficult circumstances, rather than ethical problems, hinder nurses from acting as they would like and are the most important cause of moral distress. Several authors concluded that these situations lead to feelings of powerlessness, frustration, anger, dissatisfac- tion, and exhaustion (Martin, 1989; Carpenter, 1991; Erlen and Frost, 1991; Uden et al., 1992; Erlen and Sereika, 1997; Penticuff and Walden, 2000; Raines, 2000; Oberle and Hughes, 2001; Rodney et al., 2002; Varcoe et al., 2004). Sometimes these situations cause burnout or even cause nurses to leave the nursing profession altogether (Car- penter, 1991; Oberle and Hughes, 2001). Only one study (Dierckx de Casterlé et al., 1997) examined the relationship between ethical reasoning and the implementation of ethical decisions in practise. This study reported a small but positive and significant relationship between ethical reasoning and ethical beha- viour (r = .18; p < 0.0001), indicating that the chance that nurses implement an ethical decision in practise tends to increase as their ability to make ethical deliberations increases.
- 123. 4. Discussion 4.1. Conceptual and methodological issues Most of the studies reviewed by Ketefian (1989) were based on Kohlberg’s theory on moral development and on the quantitative paradigm. The international character of this review as well as our inclusion of qualitative, quantitative, and mixed-method studies allows us to present a fairly balanced picture of how nurses actually reason and behave ethically. This review, which analysed a large number of qualitative studies and is mainly based on the experiences of nurses themselves, provides insight into the processes underlying nurses’ ethical reasoning. In the quantitative studies, many different frameworks were used and only a few studies relied on Kohlberg’s Moral Development Theory. Because of the legitimate critiques of his neglect of other elements such as context and emotion the study of Dierckx de Casterlé et al. (1997) added a caring perspective as well as some personal and situational variables in the application of the rigid, abstract justice- oriented theory of Kohlberg. Ethical behaviour is examined in a far more limited and almost indirect way, focusing on contextual factors related to ethical behaviour that either enhance or inhibit this behaviour. This finding illustrates the difficulty of actually measuring ethical behaviour. Only one study (Dierckx de Casterlé et al., 1997) alluded to the link between the reasoning and behaviour processes. This limited outcome makes it difficult to understand the relationship between ethical reasoning and ethical behaviour. When interpreting the results of this review, research- ers need to consider some methodological shortcomings. The use of various theoretical frameworks, concepts, and
- 124. definitions, and the unclear conceptualisation of the concepts ‘ethical reasoning’ and ‘ethical behaviour’ lead to highly fragmented research material that is difficult to compare and integrate. A large variation in sample sizes and response rates, possible non-responder bias, and validation of the instruments restricted to small popula- tions can limit the representativeness of results. Moreover, by selecting mainly ethically competent nurses, many qualitative studies may have presented an unrealistically favourable or optimistic picture of nurses’ ethical practises. Also, several studies were conducted in diverse research- ing settings. Although this can be viewed positively as reflecting different nursing cultures and positions in care settings, a large diversity of research settings also makes it even more difficult to clearly understand the ethical practises of nurses. 4.2. Substantive findings On the basis of our concern for the difficulties nurses face as they endeavour to apply their ethical dimension of care, we wanted to address in this review how nurses reason and how they implement ethical decisions in practise’. Nurses’ ethical practise is a difficult and complex process, in which an intricate web of personal and contextual factors plays an important role in the reasoning and behaviour processes. Most of the studies we analysed, from their own perspective, provided us with insight into the complexity of ethical practise and the difficulties that nurses face when they are involved in ethical reasoning and/or ethical behaviour. The ethical reasoning process is complicated mainly by the numerous factors that influence the ethical decision-
- 125. making process. As a starting point, nurses first consider their own ethical stance. However, they must eventually consider the values and expectations of patients, patients’ families, and others, in addition to the rules and routines of their ward and institution. Due to these influencing factors, nurses experience various difficulties that hamper their personal decision-making process. Indeed, numerous factors can hinder nurses from applying their ethically desirable decisions to clinical practise: stressful work environment, limited time and resources, lack of partici- pation in the ethical decision-making process, confronta- tion with opposing values and norms, and willingness to conform to the expectations of others. As a result, nurses are more likely to conform to the decisions of others. Especially the difficult working conditions prevent nurses from acting ethically. The impact of the context on nurses ethical practise is not only supported by studies S. Goethals et al. / International Journal of Nursing Studies 47 (2010) 635–650 647 that rely on Kohlberg’s moral development theory. In a lot of qualitative studies in this review, collecting nurses’ narratives, indicate that the context is not only a crucial but also a problematic factor in their ethical practise. Using Kohlberg’s cognitive approach, one could suggest that nurses apply only a limited form of ethical reasoning, in which they often stick to the conventional level when faced with complex issues. Due to their central position in patient care, nurses seem to be the obvious persons to act as central figures in the ethical decision-making process. Several studies in this review show, however, that nurses are involved very little,
- 126. if at all, in this process, making it difficult for them to fulfil their role as patient advocates (Martin, 1989; Uden et al., 1992; Monterosso et al., 2005). Results from the study of Milisen et al. (2006) corroborate these findings, stating that 49% of nurses do not perceive themselves as having a pivotal position in care. These findings are disappointing. Because of their unique advocacy position in care, nurses are privy to crucial patient information that can contribute to a more person-oriented care. In this context, Peter et al. (2004) pointed to the lack of clarity about the responsi- bilities delegated to nurses. Because of their accessible position in the care system and because they are driven by their feelings of responsibility towards patients, nurses often take over additional responsibilities from other care workers. As a result, nurses are faced with more responsibilities than they can reasonably handle with the time and resources available. Such situations cause nurses to feel like ‘task-oriented technicians’ rather than the ‘caring professionals’ they would like to be. These findings help us to understand why nurses, in the context of ethical practise, experience an unbridgeable gap between what they would like to do and what they only can do in practise. The qualitative studies we reviewed especially demon- strate that nurses want to behave in a patient’s best interest, while many of these studies highlight the difficulties nurses face when they want to reason and behave in the patient’s best interest. Nurses are inclined to follow their intuitions and feelings, whereby ‘care’ and ‘doing good for the patient’ are the main motifs motivating their behaviour. The multi-facetted meaning of the concept ‘nursing care’, as sketched by Gastmans et al. (1998), provides insight into the motifs driving nurses’ actions. We consider
- 127. ‘good care’ to be both a praxis and a moral endeavour, in which attitudes and activities are the essential inalienable components of nursing practise. This presupposes a caring relationship between nurses and patients expressed in a caring behaviour which is both technical accomplished and virtuous. The development of a caring relationship with the patient, which is in most cases reciprocal, is essential for nurses’ ethical practice (Gastmans et al., 1998). A reciprocal relationship positively affects the mental well-being of nurses and results in feelings of satisfaction and person growth, and leads to renewal (Finfgeld-Connett, 2007). To which extent can nurses give meaning to and experience satisfaction in their job given the difficult circumstances in which they work? The results of this review, which show how difficult working condi- tions prevent nurses from acting ethically, are supported by a large body of international literature demonstrating that difficult working conditions do indeed have an impact on nurses and patient care (Aiken et al., 2001; Peter et al., 2004; Gutteriez, 2005; Nordam et al., 2005; Milisen et al., 2006; Torjuul and Sorlie, 2006; Pendry, 2007). This suggestion is particularly unfortunate when nurses feel so unhappy with their job situation that they are compelled to leave the profession, even though many patients need their good bedside care (Peter et al., 2004; Gutteriez, 2005; Milisen et al., 2006). However, Vogel Smith (1996) also showed that good cooperation with physicians is also important. Yet several studies examined in this review showed that nurses experience poor cooperation with physicians. This finding is consistent with the findings of Siebens et al. (2006) in which 43.3% of nurses reported a lack of teamwork between physicians and nurses. Larson (1999) concluded that lack of collaboration, coordination, and shared decision making between physicians and nurses leads to