

Recommended
More Related Content
What's hot
What's hot (20)
Similar to PID "Pelvic Inflammatory Disease"
Similar to PID "Pelvic Inflammatory Disease" (20)
Recently uploaded
Recently uploaded (20)
PID "Pelvic Inflammatory Disease"
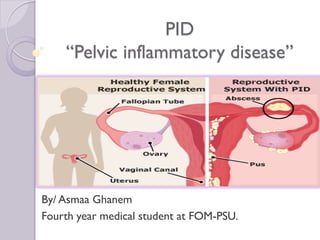
- 1. PID “Pelvic inflammatory disease” By/ Asmaa Ghanem Fourth year medical student at FOM-PSU.
- 2. Definition Etiology Types Acute PID Chronic PID
- 3. Definition PID is a clinical spectrum of infection that may involve one or more or the following structures: (7) The cervix (cervicitis), the endometrium (endometritis), the fallopian tube (salpingitis), the ovary (oophoritis), the uterine wall (myometritis), the uterine serosa and broad ligaments (parametritis), and the pelvic peritonium (peritonitis). Infection & Inflammation of the upper genital tract i.e. Tubes, ovaries, pelvic peritonium (+/- uterus) 2-3% of population. Types Acute last 2-3 days Chronic
- 4. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Chronic PID
- 5. ChronicAcute 1) Sequelae of acute PID (inadequate TTT / neglected cases) 2) Chronic from the start Polymicrobial infection Caused by 1. STDs 2. Non-specific 3. Chronic granulomatous ( TB ) 1. Primary : STDs (sexually transmitted) Chlamydia trichomatis (60%), Neisseria gonorrhoeae (40%) 2. Secondary : non-specific (normally found in vagina) I. Aerobic II. Anaerobic (Mixed) Etiology Organism Predisposing factors Routes of infection
- 7. 2 STDs Gyna 2 Obst Must open to pass the organism 1. Mucous mem &cilium 2. Wall 3. Peritonium (except)
- 8. Etiology Organism Predisposing factors Sexually active females with multiple sexual partners (usually after menses “loss of cx plug, degenerated endometrium, retrograde menstruation”) IUCD users (Barriers + COC PID) Recent instrumentation of uterus (D&C /HSG ) Routes of infection Ascending “Endogenous” through: Lumen endosalpingitis Lymphatics interstitial salpingitis Direct neighboring organs perisalpingitis Blood “Hematogenous” T.B. endo-, interstitial, peri- salpingitis
- 9. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Etiology Pathology Clinical picture DD Investigations Complications TTT Chronic PID
- 10. Etiology: 1. STD's Chlamydia trichomatis (60%), Neisseria gonorrhoeae (40%) 2. Puerperal or post-abortive 3. Non-specific organisms (aerobic or anaerobic): usually mixed Pathology: a) Acute catarrhal salpingitis - Resistance: high - Infection only of m.m. serous exudate in lumen - Fate complete resolution b) Acute suppurative salpingitis - Virulence: high - Infection (Pus) to all layers purulent exudate in lumen - Fate chronicity, spread (pelvic peritonitis) c) Acute perisalpingitis fimbrial adhesions closure of fimbrial end. If Obstruction: Partial ectopic, Total infertility 1- resistance of host 2- virulence of organism
- 11. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Etiology Pathology Clinical picture Investigations Complications DD TTT Chronic PID
- 12. congestive symptoms : (according to site) 1- Pain Vagina: dyspareunia Uterus: dysmenorrhea Rectum: dyschezia (painful defecation) Bladder: dysuria Back: dorsal pain Abdomen : deep aching abdominal pain 2- Bleeding Uterus: menorrhagia Ovary: poly menorrhea 3- Discharge Odorless : (non-infected) Leucorrhea Offensive : infection, pus, purulent, mucopulurent Investigations 1- Organism: C & S Culture+smear Ag detection Serology 2- Organ: C B C Culture Blood See (U/S, Laproscopy)
- 13. Clinical picture 1) Symptoms (history of PDF +) • General FAHM-R • Abdominal acute lower abdominal pain • Pelvic congestive symptoms (pain, bleeding, discharge) 2) Sings • General signs of infection (pulse, Tm, look toxic) • Abdominal tenderness & rigidity in lower abdomen (peritonitis)* maximum 3 cm above mid-inguinal point (tubal point) • P/V tender movement of cx, tender adenexae +/- tender mass Bimanual ex (T only no mass), Speculum ex (discharge). ALL SYMPTOMS ARE NON-SPECIFIC
- 14. Investigations: Culture: swab from 1ry &2ndry sites (Chlamydia invade single layer columnar cells) endocervix, Bartholin G, Skene’s Gland, rectum, pharynx. Blood: ESR, TLC, CRP differentiate Acute from Chronic Complications: (see the infection) U/S: TOA “Tubo-ovarian abscess”, Adnexal swelling. DD *Teratoma *Ectopic pregnancy *inflammatory Laparoscopy: GOLD STANDARD red, swollen, edematous tube (+/- mass) pus may exudate from fimbrial end cytology Criteria for diagnosis
- 15. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Etiology Pathology Clinical picture Investigations Complications DD TTT Chronic PID
- 16. Complications 1- Chronicity, recurrence (deep racemose gland of cervix, antibiotic does not reach it). 2- Obstruction: of tubes leads to Infeftility, Ectopic pregnancy 3- Spread: “septic focus” - Pelvic abscess formation - Thrombophlebitis - Peritonitis - Septicemia
- 17. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Etiology Pathology Clinical picture Investigations Complications DD TTT Chronic PID
- 18. Treatment Prophylaxis 1- Avoid SIDs 2- Aseptic techniques 3- Early diagnosis Active 1- General lines .. If diffuse inflammation NOT localizes & abscess. (Antipyretics, Analgesics, Antibiotic), rest “Fowler”, partner TTT 2-Antibiotic therapy: in combination (continued 48 hrs after resolution of fever) o Regimen I.......cefoxitin (2nd) or cefotaxime (3rd) + Doxycycline o Regimen II... .. .clindamycin + gentamycin o Regimen III...ampicillin + gentamycin + metronidazole (triple antibiotic) 3- Hospitalization: - Nulliparity or low pariry to avoid infertility - Bad general condition (*large mass :TO mass, *complicated mass: ruptured) 4- Surgical intervention: If * Severe, medical ttt failed * ruptured /huge TOA*generalized peritonitis Laparotomy + drainage + peritoneal toilet (+/- Unilateral adenxectomy), Pelvic clearacne (TAH+ BSO) *If small tuboovarian abscess aspiration (U/S guided or Laparoscopy) *Pelvic abscess drain by posterior colpotomy *Thrombophlebitis heparin 5- TTT of specific organism:
- 19. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Chronic PID Etiology Pathology Clinical picture DD Investigations TTT
- 20. Pathology: (5) 1) Hydrosalpinx: Acute catarrhal salpingitis * Serous fluid, thin wall, mild adhesions + pelvic pressure & pain. * More: torsion, infection, rupture. HSG = retort shaped swelling 2) Hydrosalpinx + Inflammatory ovarian cyst = Tubo-ovarian cyst 3) Pyosalpinx: Acute suppurative salpingitis * Thickened tube, full of pus, dense adhesions * Less torsion. HSG = smaller in size 4) Pyosalpinx + ovarian abscess = Tubo-ovarian abscess 5) Perisalpingitis : Acute perisalpingitis 6) Salpingitis isthmica nodosa (chronic interstitial salpingitis) * Thickened, interstitial abscess, Obstruction Multiple bilateral nodules & diverticula (esp in isthmus) 7) Fitz-Hugh-Curtis syndrome * Perihepatitis associated with chronic PID. C/P recurrent upper right abdominal pain. Inv. laparoscopy violin string-like bands of adhesions.
- 22. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Chronic PID Etiology Pathology Clinical picture DD Investigations TTT
- 23. Clinical picture 1) History: previous attacks of acute PID or ectopic 2) Symptoms o Infertility o congestive symptoms o Recurrent acute exacerbations 3) Sings General: ill health TB toxemia. Abdominal: sings of TB peritonitis or bilharziasis HSM Pelvic: *tenderness (Lower abdominal, cervical motion) * TO (adenxal) mass *Fixed RVF DD: Endometriosis, cancer ovary, TB
- 24. Definition Etiology Organism Predisposing factors Routes of infection Types Acute PID Chronic PID Etiology Pathology Clinical picture DD Investigations TTT
- 26. Definition Etiology Types Acute PID Chronic PID Pelvic abscess